
Table of Contents
If you have knee pain, this case study is a MUST to see
Does your knee cap point inward but your foot? point outward?
If so, then you MUST check out this post because we outline a critical factor with this postural presentation:
A “twisted” knee occurs for different reasons in different people.
I’ll illustrate why by checking out this wide infrasternal angle case study below. You’ll find that the way this person does it is different from other folks.
Check it out below. Also, if you want to see the other case, you can find that here.
Why does the knee appear twisted?
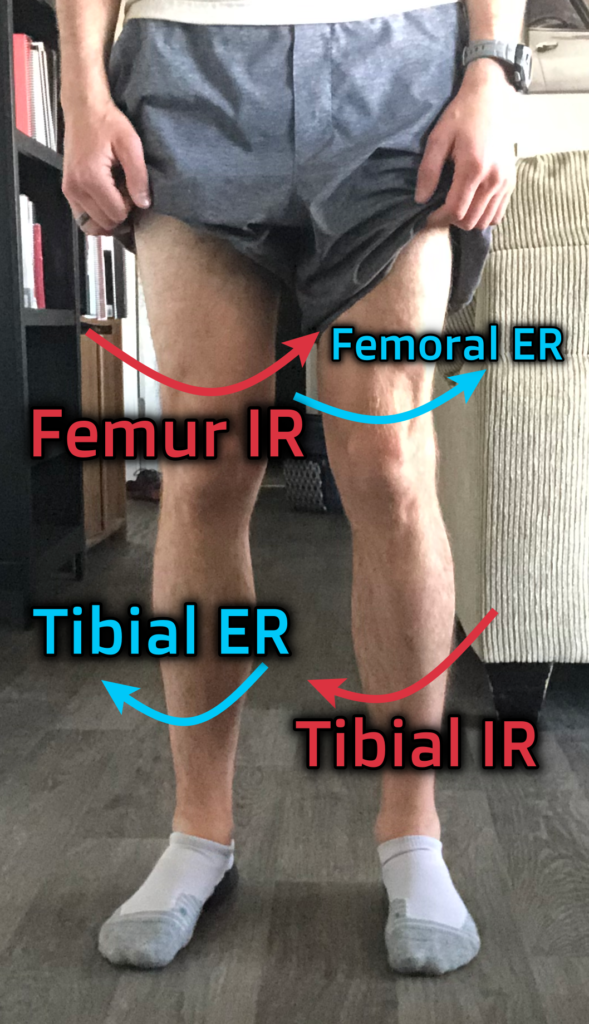
Generally, A knee will appear twisted when you have the following combination:
- Femoral internal rotation
- Tibial external rotation
And it looks like this:
But here’s the deal, the components that create this twist occur differ among individuals. In fact, these are but a few of the factors that could contribute to the twist:
- Left hemipelvis anteriorly tilting
- Pelvis translating forward
- Pelvic rotation
- Distal femur ONLY internal rotation
- Tibial torsion
- Proximal tibial ONLY externally rotating
- Others I can’t think of off the top of my head
To illustrate how this can occur, we will look at two different cases, and how the “same” problem can require different solutions.
Wide infrasternal with knee twist
Let’s now look at a way one with a wide infrasternal angle has twisted his knee.

If you look at this gentleman’s knee posture, you can see a lot more bowing of the legs, with the kneecaps twisted a bit more inward (more right than left).
But the way the twist is occurring is bit different than what we’ve seen with the narrow in our previous post. Let’s look at this person’s measures:
| Test | Left | Right |
| Infrasternal angle (ISA) | Wide | Wide |
| Active Straight leg raise (ASLR) | 100º | 110º |
| Hip flexion | 115º | 115º |
| Toe touch | Palms floor | |
| Hip external rotation | 70º | 60º |
| Hip internal rotation | 20º | 30º |
If you’ve followed me for a minute, you’ll recall that a Wide ISA should NOT have a bunch of external rotation, yet here we are. This guy is externally rotating like a boss.
Or so it seems.
Check out his foot posture and side profile of his legs:

You can see that he has some knee hyperextension coupled with the toes a bit more scrunched together.
Given all of these measures, you are likely seeing someone who is translating the pelvis forward to the point where you have a posterior tilt/orientation through the lumbar spine. The former is demonstrated by the hip rotation measures, knee posture, and foot posture. The latter is indicated by the ASLR and toe touch being so flexible. These will be the first priorities.
Now, you’ll also notice the slight asymmetry in hip rotation. This posture is likely indicative of the pelvis turning right on an oblique axis but is not the first priority.
For this presentation our focus will be as follows:
- Pull pelvis backward WITHOUT anteriorly orienting
- Drive some internal rotation to reduce posterior orientation through lumbar spine
- Progress through oblique axis protocol
The first two moves I would be starting with would be some type of elevated quadruped position without a tuck. A rollout variation would be prime here
Followed by a bent over sink squat:
Once we’ve established that this person can do this (Some IR restored), we need to progress his ability to internally rotate without anterior orientation. You could make this happen by working on something like a bent over step up, which if the knee is kept centered could actually help with the knee untwisting we need:
Then progress this to a superhero split squat for even more depth:
Once you are here, pending what ranges of motion are left, you can go through addressing the oblique axis representation, which for that, here is the four-step sequence I’ve been using:
- Stack (we did that above)
- Expand right posterior (we likely did that with the above)
- Push right to left
- Left orientate the pelvis, push right to left
Since we addressed steps 1 and 3, let’s look at what 3 and 4 could be. For pushing right to left, we can use lateral squats:
Then for 4, I’d be looking at a right split squat first, making sure we keep the right knee centered. This could actually help us quite a bit with “untwisting” the right knee:
Then last, we could combine pushing fully left with untwisting the left knee, using this terminal knee extension variation:
Sum up
Those would be the ways I would address this specific case.
To recap:
- A twisted knee occurs with femoral internal rotation and tibia external rotation
- If from a wide presentation like this, we would pull hips back, restore internal rotation, and address oblique axis.
What struggles have you had with knee problems? Comment below and let the fam know!