Table of Contents
Y’all Wanna See a Dead Body?
I remember my first cadaver dissection way back in undergrad. My first time seeing what the body “actually” looked like, not a two-dimensional representation.
Exploring the human body via dissection left an indelible mark on my anatomical understanding. There is something incredibly salient about holding a human heart that the donors so graciously provided. It took my understanding to another level.
I had a few other times in undergrad and PT school where I was able to study cadavers, but that was 8 years ago. My lens has changed. My biases have been altered. My appreciation for the human body and relationships is different.
In PT school, dissection time is basically 75% fat removal, 20% separating structures, and 5% appreciating. Especially considering the primary objective is rote anatomical memorization for the test, you don’t get to take time and stop and smell the formaldehyde.
You do what you gotta do to get that degree, fam.
This dissection I got to participate in was hosted by University of St. Augustine. Without the pressures of PT school and better anatomical knowledge, the experience was worthwhile. A breath of fresh…well you know what I mean.
It didn’t hurt that anatomical genius Daddy-O Pops Bill Hartman was in the heezy.
We had pretty much free reign on these cadavers, which allowed see so many cool things, reinforce many ideas, and develop greater understanding of how to apply anatomy to our advantage.
Realize that this post is horrendously biased. There is a certain frame of reference in which I am looking at the body and movement, and I can only speak from that reference. But my hope is that some of my takeaways either prove useful or spark thought and discussion.
Enjoy!
The Body is Continuous
Dissection involves separating specific structures apart from one another.
Pre-separated, however, good luck delineating what is what. Muscles, tendons, ligaments, fascia are quite interconnected, as though they are one piece. The tissues are starkly different the further into the dissection, but before that not so.
Hell, it can even be challenging separating muscles. After seeing the fingerlike transverse process attachments of the levator scapulae (which was way cool), you could see how continuous this muscle was with the rhomboid and serratus anterior.
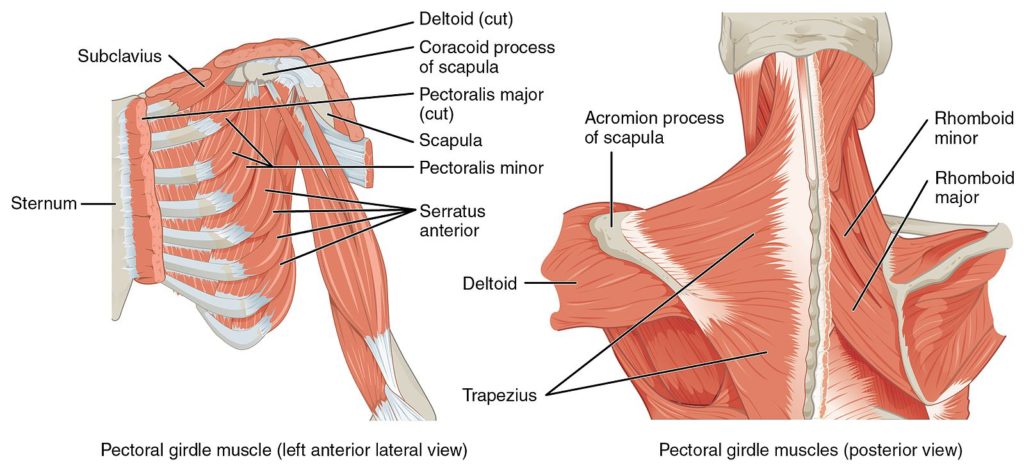
Though focusing on specific tissues can simplify understanding and in some cases can guide treatment, reductionism is not the reality.
You really think you are palpating the psoas? Think again. You sure that’s the soleus? Maybe it’s an accessory soleus (we had a cadaver with an extra one in our class). Or maybe it’s fascia? Or maybe you aren’t even close because the fam you are working with has subcutaneous fat like whoa.
When you see the inside of the human body, you will be humbled. You will question if you are actually doing what you think you are doing, and you will leave uncertain.
The Myth of Fusiform Muscles
A fusiform muscle is defined as one in which muscle fibers are parallel to one another1.
Helpful definition, but too bad they don’t exist.
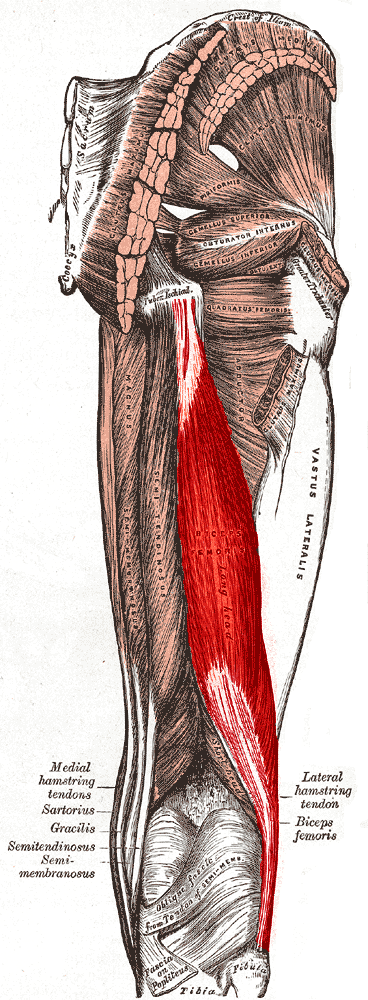
I looked at quite a few muscles, and one thing I noticed was that all of the muscle fibers had a curve to them. The hamstrings, a de facto “fusiform muscle,” curve from their proximal to distal attachment. The adductors sharply curve on their way to attaching at the pubis. the triceps curve to their attachment at the elbow.
Curve, curve, and more curve. That’s all I saw.
After attending Daddy-O Pops’ The Intensive and seeing these curved muscles, I am questioning more if we ever could possibly operate in a singular plane of movement. Perhaps, like breaking things down to specific tissues, planes are a language of convenience more so than a reflection of what is actually occuring.
Breathing Debunked
Of course, you know that big Z is going to take a look at as many breathing-related pieces of anatomy as possible.
The most impressive thing Pops and I got to dissect out were the crural attachments of the diaphragm.
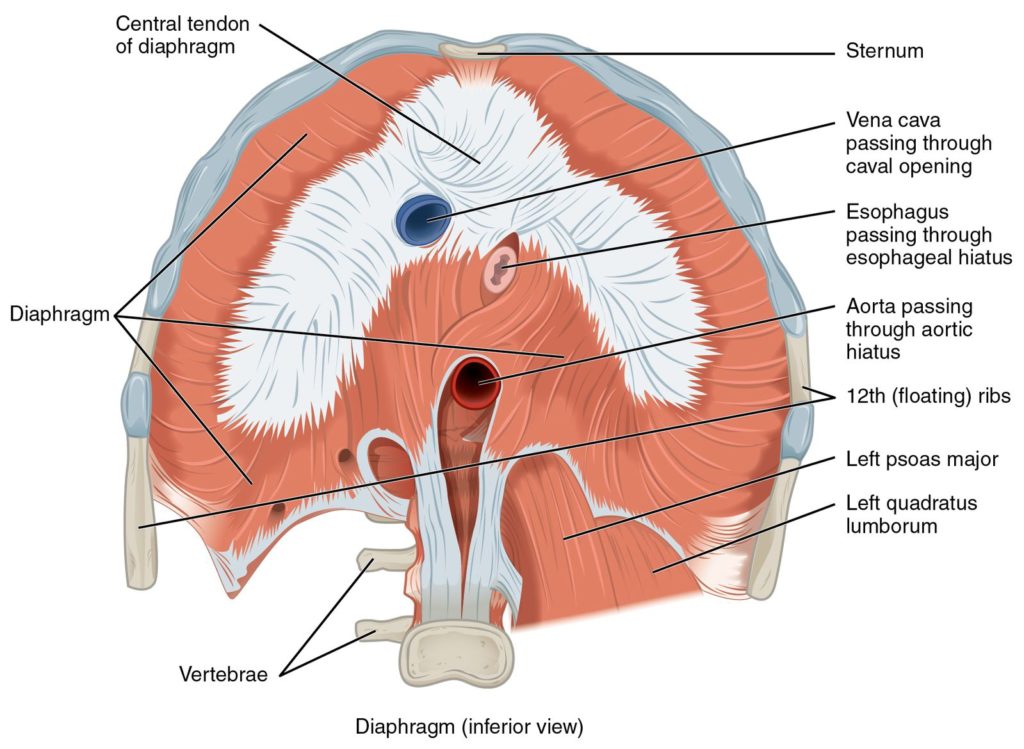
First off, these tendons are thick and dense, which means the diaphragm likely has a bigger influence on the spine than we likely think.
The diaphragm’s actions on the spine, however, aren’t what some may think. The crura were pretty much front and center on the vertebral bodies. This locations suggests that the diaphragm primarily extends the spine, but has minimal rotational influence. The evidence seems to suggest similarly2.
We also got to check out some dopeness surrounding the sternum. The intercostal delineation was quite fascinating. If you compare external versus internal intercostals, you can clearly see where the externals ends (about 3-4 inches from the sternum) and the internals begin right on the sternum).
If you break down anatomical function, the external intercostals are conventionally taught to be inhalers, whereas the internal intercostals are thought to be exhaler muscles.
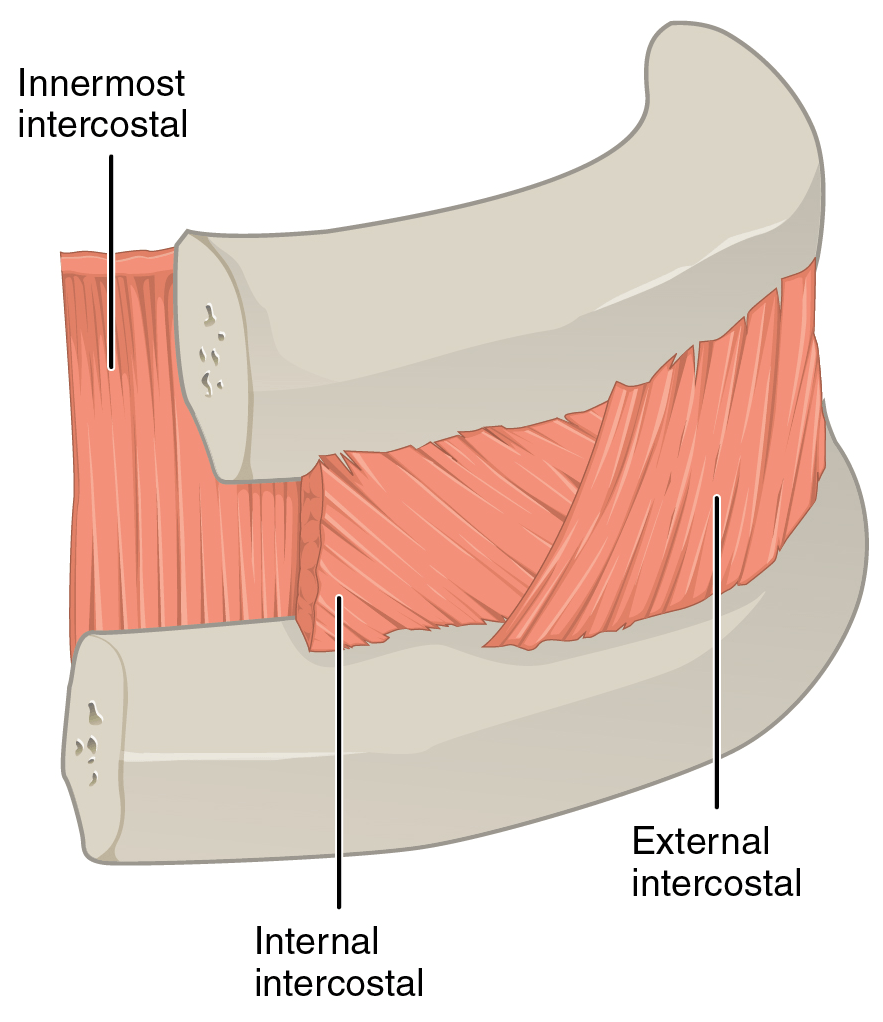
Riddle me this though, how would the internal intercostals help with exhalation around the sternum when they sit anteriorly? Exhalation near the sternum is handled by triangularis sterni (which spoiler alert, is NOT always asymmetrical in number)?
The answer: anatomy textbooks are wrong. The internal intercostals near the sternum, called the parasternal intercostals, have an inhalation function. These muscles both create the pump handle action of the anterior ribcage and prevent excessive diaphragm descension. What determines intercostal function is not specific muscles, but neural drive and location. Intercostals that are on the anterior and posterior aspects of the ribcage have greater inhalation capabilities, while those which are lateral assist with exhalation3.
You Gotta Have Guts
After spending some time with Daddy-O Pops, the guts have become fascinating. A structure we probably don’t consider as having much impact on movement.
But these bad boys are huge, mobile, and asymmetrical. I mean, check out where the mesentery attaches, aka the mesenteric root. This attachment site runs from the left side of L2, then goes obliquely to the right SI joint4.
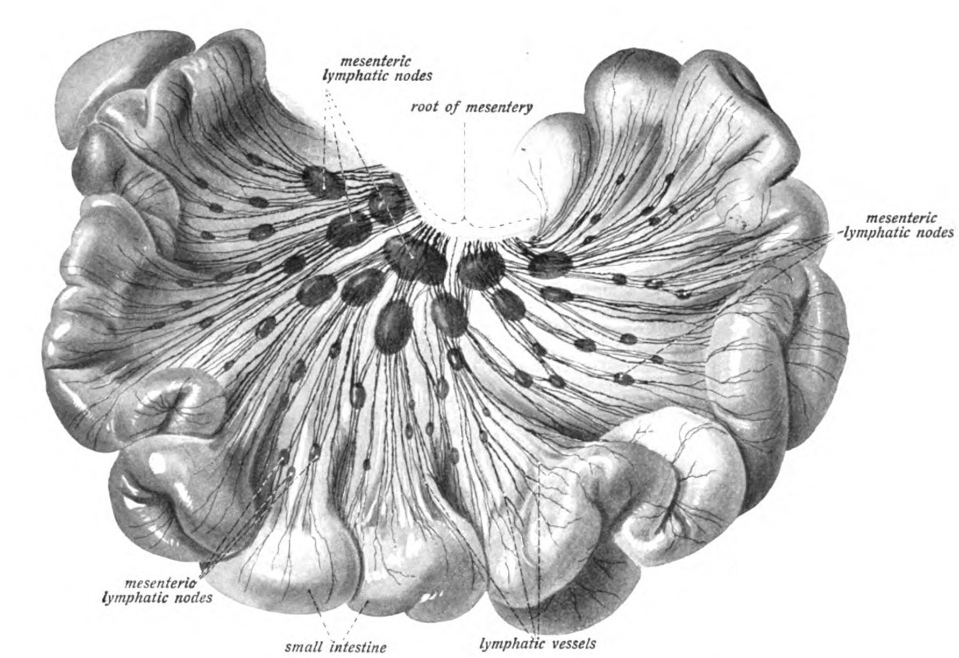
Think about what implications this may have on movement, asymmetry, and many other things. The fact that the guts move when intra-abdominal pressure is increased makes me wonder what implications this asymmetry has on our movements capabilities. Stay tuned.
Sum Up
Cadaver dissection was an incredibly worthwhile experience, and if you ever get a chance to attend, I strongly encourage it.
To summarize:
- All body structures contain some degree of continuity, and likely work together to get us to do what we do
- All muscles have a degree of curve to them
- The diaphragm’s crural attachment likely help with lumbar extension
- Intercostal action based on location
- The guts are asymmetrical and likely influence are movement capabilities
If you’d like to learn how to apply some of the material that I learned from my dissection, you’ll definitely want to check out Respiration Revisited and Breathing Mechanics 101.
Have an experience with cadaver dissection? What did you learn? Comment below and let the fam know!
References
- Fusiform muscle on Sciencedirect
- Hudson et al. Role of the diaphragm in trunk rotation in humans. 2011. J Neurophysiol;106(4):1622-8.
- De Troyer. Mechanics of the respiratory muscles. 2011. Comprehensive Physiology;1(3):1273-1300.
- Okino et al. Root of the small-bowel mesentery: correlative anatomy and CT feature of pathologic conditions. 2001. Radiographics;21(6):1475-90.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}