
Table of Contents
Your tuck isn’t what you think it is
You’ve been all excited about teaching everyone to tuck their hips during exercise, then it happens:
“Coach, my back HURTS!!!! WTF?!?!”
That tucking must be a bunch of bs then, right?
FALSE!
Many peeps have a markedly difficult time differentiating pelvic motion (aka what is needed during the tuck) vs lumbar flexion (a common compensation seen when tucking).
When you “tuck” using the lumbar spine, there is no change in the pelvic floor orientation, reduced leg activity, and increased spinal load, which can be straining on some of your favorite lifts.
Want to know the difference and how to make your tuck feel great!?
Then check out Movement Debrief Episode 140 below!
Watch the video below for your viewing pleasure.
Or listen to my sultry voice on the podcast version:
If you want to watch these live, add me on Instagram.

 t
tShow notes
Check out Human Matrix promo video below:
Below are some testimonials for the class:
Want to sign up? Click on the following locations below:
February 20th-21st, 2021, Atlanta, GA (Early bird ends January 17th at 11:55 pm!)
April 10th-11th, 2021, Warren, OH (Early bird ends March 14th at 11:55 pm)
May 29th-30th, 2021 Boston, MA (Early bird ends April 25th at 11:55 pm!)
August 14th-15th, 2021, Ann Arbor, MI (Early bird ends July 18th at 11:55 pm!)
September 25th-26th, 2021, Wyckoff, NJ (Early bird ends August 22nd at 11:55 pm)
November 6th-7th, 2021, Charlotte, NC (Early bird ends October 3rd at 11:55 pm)
Dickinson College in Carlisle PA (POSTPONED DUE TO COVID-19) [Approved for 14 Category A CEUs for athletic trainers]
Montreal, Canada (POSTPONED DUE TO COVID-19) [6 CEUs approved for Athletic Therapists by CATA!]
Or check out this little teaser for Human Matrix home study. Best part is if you attend the live course you’ll get this bad boy for free! (Release date not known yet 🙁
Here is a signup for my newsletter to get nearly 5 hours and 50 pages of content, access to my free breathing and body mechanics course, a free acute:chronic workload calculator, basketball conditioning program, podcasts, and weekend learning goodies:
[yikes-mailchimp form=”1″ submit=”Get learning goodies and more”]
Hip flexion debriefs – If you want to deep dive into hip flexion, then you’ll need to check this out.
Improve your hip flexion like a boss with this move:
The rockback hip extension is a progression from this.
The difference between sacral counternutation and lumbar flexion
Question: Hello Big Z!! I hope you are doing well. I have a question I hope you could talk about a little.
Could you explain the difference between sacrum counternutation and the lumbar spine/pelvis flexing as a unit?
What should be looking at in a client? Is it possible to see the difference?
Thank you as always, for all the teaching you do. It does make a huge difference!
Answer: The big difference between these two strategies is:
- Sacral counternutation changes pelvic floor orientation
- Spinal flexion can occur without changing pelvic floor orientation
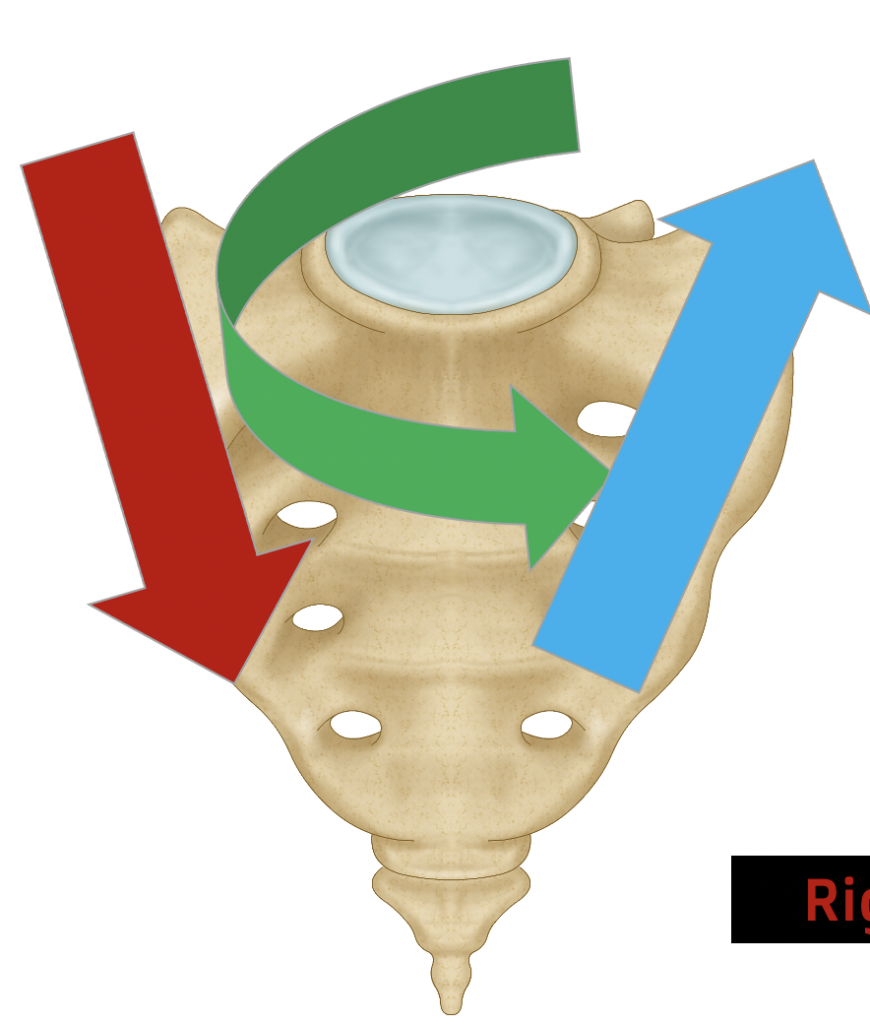
With sacral counternutation, the posterior pelvic floor concentrically orients, and the anterior pelvic floor eccentrically orients. You will also have a concomitant reduction of lumbar lordosis (some spinal flexion) that is oftentimes uniform.

Visually, when this is performed, you will see a subtle reversal of lumbar lordosis, with minimal hinging at specific segments in the lumbar spine. Counternutation will visually look like superior and inferior pelvic motion.

We typically do not see this with isolated spinal flexion. Usually, this action occurs as a compensatory strategy when someone cannot alter pelvic floor orientation.

Instead, the person will typically flex at a particular segment or two within the lumbar spine. You may see one part of the lumbar spine bulge out when someone does this action. Visually, the pelvic will move more in an anterior direction.

This strategy is undesirable because it can increase strain in particular segments in the lumbar spine. The lack of changing pelvic floor orientation will also reduce the contribution of glutes and hamstrings to the movement, as rectus abdominis becomes the predominant tucker. If you are someone who attempted to make your squat more squatty and your back hurt as a consequence, this compensation is a probable reason for it.
The solution is to drive more sacral counternutation with your tuck. There are a few different verbal cues that I like which helps attain this position:
- Back pockets to heels
- Pubic bone to nose
- Buttflap to thigh
- Tuck with abs relaxed
If someone is still strugglebus when it comes to this strategy, having them arch their back, then un-arch their back slowly usually will clear this cheat up.
Hip pinching at the bottom of a squat
Question: I’m struggling with deep hip flexion and it feels like I’m “blocked” or pinched in the front of my hips when I try to sit deep in a squat or at the setup position for a barbell snatch.
I noticed when I am good about prepping with your Wall Stride breathing that you gave me, I’m more comfortable in those positions, but it still feels somewhat blocked.
It seems that hip flexion issues are complicated, but I wanted to try and make a little sense of it if possible and see if you had any resources.
Answer: There are only about 120 degrees of hip flexion available. YET, peeps can squat well into 145 or even 150 degrees.
HOW IS THAT EVEN POSSIBLE?!?!!?
The answer, folks, is relative motion. As you progress through deeper hip flexion, there is a relative movement at the pelvis, sacral counternutation, that assists in hitting depths beyond what the femuracetabular joint allows.
This concept of relative motion is the same reason you can go fully overhead with your arm, yet only 120 or so degrees of it comes from the glenohumeral joint proper. So-to with the pelvis.
Therefore, full thigh to abdomen hip flexion can only occur if the sacrum can counternutate.
If this relative motion is absent, pressure will buildup in the anterior portion of the femuroacetabular joint at the end of available hip flexion, often creating a sense of pinching of blocking.
The fix? Increase your counternutation skillzzz!
I sequence improving sacral counternutation in a 4-step process.
The first step is to increase sacral counternutation by working on squat progressions. Ramp squats work great for this:
If bilateral counternutation efforts don’t do the trick, then you have to begin rotating the sacrum. When I perform hip flexion unilaterally, the sacrum will have to rotate towards the flexed leg. This will present with increased counternutation ipsilaterally relative to a bilateral action.
Performing asymmetrical exercises like the wall stride are great ways to initiate this process:
But sometimes even this movement isn’t enough. Now is the time to introduce hip shifting-based exercises to complete the action.
An early phase hip shift is more frontal plane in nature, mimicking pelvic position in midstance. The pelvis will appear at an oblique angle (one side higher than the other). The table side stride is a great choice for this:
If you want to push the envelope even further, you’ll need to do a full-blown hip shift, actively rotating the sacrum towards the side in question. A posterior hip stretch is a prime example of this action:
If you go through this progression, there’s a good chance that your hip flexion will improve, and ought to be less pinchy.
Sum up
- Sacral counternutation involves pelvic floor motion, whereas spinal flexion can occur without this motion.
- Flexion without sacral counternutation is an inefficient way to demonstrate intra-abdominal pressure.
- Hip pinching can occur when there is no relative sacral counternutation in deep hip flexion. Drive counternutation and hip shifting to restore this motion.