
Table of Contents
A deep dive into hip motions
When you see someone squatting, with hip limitations, and shifting, do you ever wonder…
What the hell is going on?
No doubt this is especially confusing when you are looking at how the pelvis moves, spine moves, throw breathing in the mix….YIKES!!!!
But what if hip movement could be simple? I think we can make this the case if we can grasp:
- How hip movements become restricted
- How hip dynamics change when we go through movements like a squat
- How we can bias certain exercises with shifting to target these specific limitations
Are you ready to take your lower body exercise programming and knowledge base to the next level? Then check out Movement Debrief Episode 128!
Watch the video below for your viewing pleasure, or listen to the podcast if you can’t stand the sight of me 🙁
and the audio version:
If you want to watch these live, add me on Instagram.

 t
tShow notes
Check out Human Matrix promo video below:
Below are some testimonials for the class:
Want to sign up? Click on the following locations below:
September 12th-13th, Montreal, Canada (Early bird ends August 16th at 11:55pm!) [6 CEUs approved for Athletic Therapists by CATA!]
October 3rd-4th, Ann Arbor, MI (Early bird ends September 6th at 11:55pm!)
November 7th-8th, Charlotte, NC (Early bird ends October 11th at 11:55pm!)
November 21st-22nd, San Diego, CA (Early bird ends October 25th at 11:55pm!)
February 20th-21st, 2021, Atlanta, GA (Early bird ends January 17th at 11:55 pm!)
May 1st-2nd, 2021, Minneapolis, MN (Early bird ends April 4th at 11:55pm!)
May 29th-30th, 2021 Boston, MA (Early bird ends April 25th at 11:55pm!)
Dickinson College in Carlisle PA (POSTPONED DUE TO COVID-19) [Approved for 14 Category A CEUs for athletic trainers]
Or check out this little teaser for Human Matrix home study. Best part is if you attend the live course you’ll get this bad boy for free! (Release date not known yet 🙁
Here is a signup for my newsletter to get nearly 5 hours and 50 pages of content, access to my free breathing and body mechanics course, a free acute:chronic workload calculator, basketball conditioning program, podcasts, and weekend learning goodies:
[yikes-mailchimp form=”1″ submit=”Get learning goodies and more”]
Hip Rotation Explained – If you want to learn how the pelvis influences hip rotation, why someone could have a hip rotation restriction, or a CRAZY amount of mobility, check this debrief out!
If you need a move that drives counternutation and spinal flexion in general, the drunken turtle is one of my go-to activities:
The position for many that I teach “the stack” in is hooklying. Try this progression:
Effect of Changes in Pelvic Tilt on Range of Motion to Impingement and Radiographic Parameters of Acetabular Morphologic Characteristics – This study shows how pelvic position influences hip joint measures. Get that stack first, fam!
Kinesiology of the Hip: A Focus on Muscular Actions – One of my favorite clincial commentaries on how muscles influence hip motions; written by the OG himself, Don Neumann.
Bill Hartman – Daddy-O Pops is one of the biggest pioneers in our field, and got me turned on to the rotational changes seen in squats and more!
A biomechanical comparison of the traditional squat, powerlifting squat, and box squat – This study illustrates how hip rotation changes during squatting with various stance widths.
If you need a hip shift that drives more pelvic external rotation, you’ll need to try this move:
If you are going after more pelvic internal rotation, then the classic sidelying hip shift is a good choice:
Pelvic orientation versus compensation
Question: In Human Matrix, a lack of humeral internal rotation suggests concentric activity of the external rotators (a secondary compensation, if I’m not mistaken). This activity is brought about by your arms returning to an orientation that makes them more useful (for hugs, yuck).
In your hip rotation debrief, however, it seems that the mechanism is a bit different. What I came away with is that limitations in internal or external rotation are brought about by orientation (via inhaled or exhaled spines).
It seems that rotation in the first scenario is limited by compensation, and the second by orientation. Am I getting that right?
Answer: First, let’s get some definitions out of the way when discussing joint position:
- Orientation: The relative position of a body area. Generally, this is a positional bias one has (e.g. anterior pelvic orientation)
- Compensation: How a body region may respond secondary to a given orientation (e.g. the femur may drive compensatory external rotation in response to an anterior pelvic orientation)
Though it’s likely orientation and compensation occur simultaneously as a grand compensatory strategy, it’s useful to think of these actions as a sequential process.
If you know the compensatory biases each infrasternal angle presentation ought to have, this makes the process WAY simpler.
Here’s the short version:
- Narrow Infrasternal Angle: Counternutated sacrum with decreased extension, adduction, and internal rotation (femur is oriented into external rotation)
- Wide Infrasternal Angle: Nutated sacrum with decreased flexion, abduction, and external rotation (femur is oriented into internal rotation)
Any deviation from the above patterns is considered compensation. To determine if the compensation is occurring at the femur vs further concentric bias at the ventral cavity, you could look at more distal measures to confirm your suspicions:
- Concentric femoral external rotation = Decreased knee extension and tibial external rotation.
- Concentric femoral internal rotation = Decreased knee flexion and tibial internal rotation.
So then aside from compensation being more common in the thorax, why do I not teach scapulohumeral rules as I do with the femurs. Two reasons
Reason 1: No time
In a two day seminar, you can only accomplish so much. I’d rather give what is most commonly seen than tell the whole story. If you want the whole story, substitute all of the above information with scapula and humerus!
Reason 2: Scapular and pelvic ER/IR ARE NOT the same
When you drive rotation at each of these bones, you get a different movement along a different axis. Peep the video below to see what I am talking about.
Femoracetabular Impingement
Question: I was wondering if you could talk a bit more about femoroacetabular impingement (FAI). What would increase it’s potential? How it would be seen in measuring? What kind of intervention should we use?
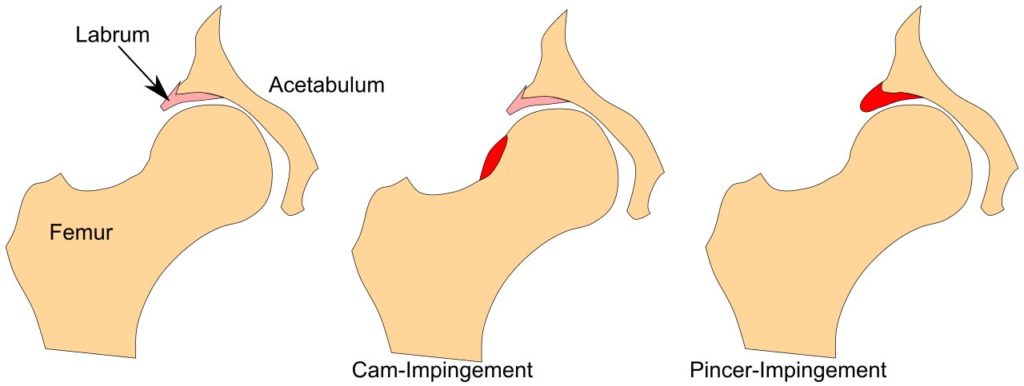
Answer: FAI is when there are bony changes within the hip joint, altering bone shape and negatively affecting biomechanics.
There exists three types of impingement:
- Cam Impingement: Extra bone growth on the femur
- Pincer Impingement: Extra bone growth on the acetabulum
- Mixed Impingement: Extra bone growth on both the femur and the acetabulum
Oftentimes, those with FAI will complain of a pinching sensation when they move their bodies into various positions. This sensation typically occurs in the direction they are moving. So if you flex your hip, you may feel a pinch in the anterior hip.
One of the most common positions is combined flexion, adduction, and internal rotation. You’ll explore this position at the midrange of a squat.
Though we as movement professionals cannot change the bony structure in this regard, we can alter body orientation to positively affect this condition.
Interestingly enough, subjects with FAI can change their available hip range of motion by altering pelvic position. That is where your focus should be: stack, squat, shift, do all the things you would normally do while avoiding any symptom reproduction.
If your client does all the good stuff savagely well, yet you see minimal change in mobility or symptoms, consider getting imaging and a surgical consult. Sometimes you have to change the structure in order to change the movement.
Hip rotation during squat
Question: You noted an inhalation/external rotation strategy for descent in a squat. Isn’t’ there relative internal rotation at the true hip joint as we get further down into a squat?
Or is the external rotation strategy just what the muscles are attempting to do for a better flow of the hip even though the bony structures are going through an internal rotation motion?
Answer: The rotational action that is occurring during the squat depends on what range of hip flexion we are discussing. There is an oscillating external rotation/internal rotation/external rotation movement throughout.
Which rotation occurs depends on several factors:
- pelvic orientation
- femoral position and rotation
- Changing line of pull of posterior hip rotators
- knee position and rotation
- Probably other shit I’m forgetting
Below you’ll see a rough breakdown of the rotational changes throughout hip flexion. The exact ranges at which these shifts occur is individual-specific, but this is a good ballpark:
- 0°-60°: external rotation
- 60°-100°: internal rotation
- 100°- Full: external rotation
Realize that these are not going from one extreme range to the other, but likely subtle directional shifts.
Therefore, if you see mobility deficits in specific rotations, you can choose exercises to address those areas or squat at differing depths to capture the mobility you oh so desire!
Hip shifting
Question: I was trying to tie the exercises you picked to mechanics and how a hip shift would bias inhalation/exhalation? Could definitely be covered in a debrief if you already haven’t!
Answer: First, you might be wondering: “Zac, what’s a hip shift big fam?!?!”
Hip Shift: rotating the sacrum in a specific direction (e.g. a left hip shift will rotate the sacrum to the left)
Much like the squat, the specific mechanics occurring at the hip shift will depend on the location the shift is occurring.
Remember this fancy flexion thing from the squat section? You read that, right? You didn’t?!? WTF?? I thought we were cool?
(Sigh), here it is again, but this time adding the sacral movement that is also occurring:
- 0°-60°: external rotation & sacral counternutation
- 60°-100°: internal rotation & sacral nutation
- 100°- Full: external rotation & sacral counternutation
Therefore, a shift at each position will bias more of the sacral motion occurring than say a bilateral move would:
- Higher depths: more counternutation
- Mid-range depths: more nutation
- Lower depths: more counternutation
So if you got a fever, and the only prescription is more nutation, you might choose a move like this:
Or if you want to be a member of counternutation nation, then I’d choose something like this:
Sum Up
- Orientation and compensation occur throughout the body, with orientation being initial bias, compensation being deviations from that bias.
- Look at multiple joints to accurately determine body position.
- FAI impacts movement by extra bone growth in the hip joint complex. Intervene as you would normally, but if no changes occur, a surgical consult is warranted.
- Squats involve an oscillation of external rotation/internal rotation/ and external rotation depending on the degree of depth attained
- Higher depth hip shifts will bias external rotation and sacral counternutation, mid-depths will bias internal rotation and sacral nutation.