Table of Contents
Can’t get overhead? Let’s figure out how!
If you can raise your arm fully overhead WITHOUT compensating, don’t read any further!
But if you are like most of us, reaching overhead probably draws its fair share of LOLZZZ.

Yet raising your arm overhead is HELLA important for things like lifting weights, moving your neck freely, and even rotation through the ribcage.
So if ya ain’t got it, you might want to work on it!
That’s why I put out this debrief for you that dives into mechanics, what directions to reach and clarifies any confusion that may surround arm elevation biomechanics.
Let’s channel our inner Josh Groban and raise you up (your arm that is).
Watch the video below for your viewing pleasure, or listen to the podcast if you can’t stand the sight of me 🙁
and the audio version:
If you want to watch these live, add me on Instagram.

 t
tShow notes
Check out Human Matrix promo video below:
Below are some testimonials for the class:
Want to sign up? Click on the following locations below:
November 7th-8th, Charlotte, NC (Early bird ends October 11th at 11:55pm!)
February 20th-21st, 2021, Atlanta, GA (Early bird ends January 17th at 11:55 pm!)
April 10th-11th, 2021, Warren, OH (Early bird ends March 14th at 11:55 pm)
May 1st-2nd, 2021, Minneapolis, MN (Early bird ends April 4th at 11:55pm!)
May 29th-30th, 2021 Boston, MA (Early bird ends April 25th at 11:55pm!)
August 14th-15th, 2021, Ann Arbor, MI (Early bird ends July 18th at 11:55pm!)
September 25th-26th, 2021, Wyckoff, NJ (Early bird ends August 22nd at 11:55pm)
Dickinson College in Carlisle PA (POSTPONED DUE TO COVID-19) [Approved for 14 Category A CEUs for athletic trainers]
Montreal, Canada (POSTPONED DUE TO COVID-19) [6 CEUs approved for Athletic Therapists by CATA!]
Or check out this little teaser for Human Matrix home study. Best part is if you attend the live course you’ll get this bad boy for free! (Release date not known yet 🙁
Here is a signup for my newsletter to get nearly 5 hours and 50 pages of content, access to my free breathing and body mechanics course, a free acute:chronic workload calculator, basketball conditioning program, podcasts, and weekend learning goodies:
[yikes-mailchimp form=”1″ submit=”Get learning goodies and more”]
All About the Scapula – This debrief goes into scapular movements during respiration, compensations, and more.
Motion of the shoulder complex during multiplanar humeral elevation – This article is essential to understanding scapulohumeral rhythm
Joe Cicinelli – He is a PT colleague of mine who is my go-to guy for all things upper airway.
Scapulohumeral rhythm
Question: Been reviewing your scapula debrief and the motions getting me a little hung up. I’ve always thought that shoulder flexion, upward rotation, ER, and posterior tilt were together? But you’re saying the scaps upwardly rotate, internally rotate, and anteriorly tilt? What’s the reasoning behind this or something I’m missing in research?
People always drove into my brain upward rotation and posterior tilt helps clear space for shoulder flexion. Any relationship or misunderstandings there?
Answer: When discussing the motion of the scapula and the humerus during shoulder flexion, it’s all about timing and location.
We typically break down shoulder flexion into 3 different phases:
- 0-60°
- 60°-120°
- 120°-180°
During these distinct phases, you have different actions happening at both the scapula and the humerus that will drive expansion into various areas.
First, we need to know what the starting position is for the scapula. “Scapman Begins” you might say…Or not…Whatever!
Most of this stuff is drawn from this article here, so please check this awesome study out if you haven’t.
The resting position of the scapula is:
- 41° internal rotation
- 5° upward rotation
- 16° anterior tip
- Humerus starts in slight external rotation
There’s going to be some slight variations among peeps of course, but this is a solid starting point.
Now, let’s look at how the humerus and scapula move throughout the three phases.
Phase I: 0°-60°
There is pretty much no movement of the scapula in this phase. It’s all humerus. No joke. (Damn I’m on fire today!)
Most of the humeral action is biased towards external rotation. If the humerus externally rotates, then the scapula will relatively internally rotate.
How do I know that? I’M GLAD YOU ASKED!!!!
It has to do with the posterior cuff muscle’s proximal line of pull.

If I contract the proximal end of these muscles to the distal attachment, you’ll notice how the medial border would lift away from the ribcage. This action, my fine fellow fam, is scapular internal rotation. Glorious, right?!
If the medial border is away from the ribcage, the scapular external rotators (rhomboids, traps, subscapularis) will be eccentrically oriented. Since the big dogs are posterior, you’ll get more posterior thorax expansion in this phase. In particular, T6-8 because of relative scapular downward rotation compared to later phases.
O°-60° = Humeral external rotation = scapular internal rotation = T6-8 posterior expansion
Phase II: 60°-120°
In this phase, the scapula has to pick up some slack to clear room for the humeral head to do its thing. So it’s gotta move!
The big scapular movements that happen during this phase are:
- Upward rotation
- External rotation
- Posterior tipping
These combined actions suction the scapula up against the ribcage, enhancing stability and reducing stress load on the cuff muscles. When you see peeps winging and whatnot, that’s typically an inability of this phase to properly occur.
Just like in phase I, scapular external rotation is associated with a relative humeral internal rotation. Peep the line of pull of your big internal rotator, the subscapularis:
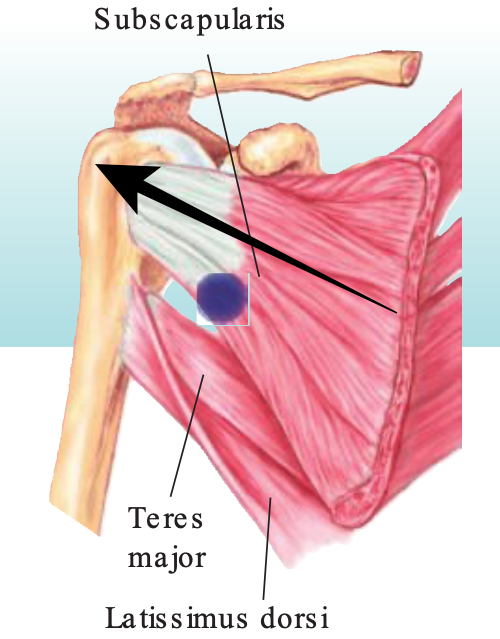
Same song and dance. Proximal pull would compress the scapula up to the ribcage, and life is good.
Due to scapular external rotation, the posterior thorax is more restricted from airflow. Thus, airflow in this flexion phase predominately occurs anteriorly. The bias is at T6-8 level in the early range, and likely T2-4 in the later range.
60°-120°= humeral internal rotation = scapular external rotation = anterior expansion (T6-8 early, T2-4 later)
Phase III: 120°-180°
The grand finale, and the most confusing part of scapulohumeral rhythm.
Scapular upward rotation, external rotation, and posterior tipping continue to happen with reckless abandon.
BUT.
There are a few major keys that happen which allow for posterior thorax expansion during this phase:
- The humerus maximally externally rotates (creating a slight internal rotation bias
- The scapula orients into the scapular plane (45 degrees anterior of the frontal plane), which positions the scapular back near the resting position (which was internal-rotation.
- the more lateral position of the scapula away from the spine increases eccentric orientation.
- The upward rotation will eccentrically bias the downward rotators (rhomboids), which have a location posteriorly
For these reasons, you will get some posterior expansion at T2-4 as you reach overhead.
120°-180°= Humeral external rotation = relative scapular internal rotation (though the scapula is still actively externally rotating) = posterior expansion (T2-4 level).
Anteroinferior glide during shoulder flexion
Question: Could you explain what to do if someone overstretched the ligaments in their shoulder. Like after doing the shoulder flexion test and their humeral head pops into your thumb when it’s in their armpit, what can I do to restore normal flexion and how can I continue to keep that person resilient?
Answer: Sometimes, when testing shoulder flexion, you can feel the humerus glide anteriorly and inferiority if you place your thumb in the client’s armpit. It’s all types of fun.
If shoulder flexion is more external rotation-bias, what I think is likely going on is a combined internal rotation and abduction action that causes this excessive gliding, hence the pop forward.
Is this actual tissue laxity? Ehhh. It’s hard to say. I’ve seen this glide change quickly with interventions, and my skills are DEFINITELY NOT that good. I think it’s unlikely a true tissue laxity, which would likely need surgical repair.
An alternative story is there is an eccentric bias of anteroinferior tissues to compensate for a lack of scapular upward rotation needed for full shoulder flexion.
You can guess the fix right? Get air in the back with a low reach, and you ought to be rocking and rolling!
I usually start with something like this:
Then progress to a single arm reach to drive rotation and more isolated posterior expansion:
Improving shoulder flexion
Question: You and others have mentioned that when someone who is compressed in the dorsal rostral thorax and it is proven with your shoulder flexion assessment between the ranges of 60°-120° among other measures, that you would intervene with low reaching exercises below 60° flexion in various positions depending on the presentation of the ISA.
Is it possible that in this instance we could intervene with a position that includes reaching in that 60°-120° degree compressive range if we IR at the humerus?
Answer: If you peeped the scapulohumeral rhythm component above (uhh, why haven’t you read that yet fam?!), you probably garnered one thing:
Shoulder flexion is hella complicated.
In fact, the entire arc of flexion involves both anterior and posterior thorax expansion to be completed.
Although I love shoulder flexion as a test, it is more a gross measure of thorax expansion with a bias towards posterior. Whereas shoulder extension is similarly a gross expansion measure with a bias towards anterior.
In order to know where you need to drive air, you have to look at segmental expansion within the thorax. Get your tight green wrestling pants on and lather up in baby oil, because we’re about to break it down Degeneration X-style.
Filling the thorax with air is similar to filling a cup of water. The cup fills bottom-up completely.

So to do the lungs during progressive shoulder flexion. The fill occurs in a sequential manner that corresponds to scapulohumeral rhythm.
Remember this general expansion trend with scapulohumeral rhythm:
- 0°-60°: lower posterior expansion (T6-8)
- 60°-120°: T6-8 anterior expansion in early phases, progressing to T2-4 expansion in later phases
- 120°-180°: T2-4 posterior expansion, with likely some anterior T2-4 expansion as well.
With that in mind, you have to look at other individual tests to determine where you have to drive specific airflow to get changes in shoulder flexion:
- T6-8 posterior expansion – shoulder external rotation at 90°
- T6-8 anterior expansion – shoulder internal rotation at 90°
- T2-4 posterior expansion – shoulder horizontal abduction
- T2-4 anterior expansion – shoulder horizontal adduction
- T2-4 anterior AND posterior expansion – Lower cervical rotation

Before you get all wild and crazy with your specific expansion efforts, make sure you have the stack.
If you don’t have the stack, you have no base to drive this segmental expansion, and you won’t be able to talk to me, and I’ll stay forever lonely. I NEED YOU FAM!
Once you have the stack, then you can pinpoint where the mobility restrictions are, then fill up your cup!
If you have decreased shoulder external rotation (less than 90°), I’d go with a reach in the 0°-60° range:
If you have decreased shoulder internal rotation (less than 90°), I’d go with a reach in the 60°-120° range:
You can combine expansion in both these areas by driving single-arm reaches. If I reach with my right arm, that will drive anterior expansion on the right and posterior expansion on the left:
If you have decreased shoulder horizontal abduction (less than 45°), I’d go with something that drives rotation with a more horizontal plane-bias. The sidelying armbar roll is a go-to for me:
If you have decreased shoulder horizontal adduction (less than 135°), you can use similar rules above and drive horizontal adduction. Short lever side planks are money here.
You can also go with humeral extension to improve this movement:
Lastly, if you want to drive anterior and posterior expansion with the upper segments, you can combine unilateral reaches with cervical rotation. The armbar screwdriver with head turns is an absolute beast-mode for this:
Manubrial Expansion
Question: How would you differentiate an overhead reaching exercise for purpose of upper anterior ribcage expansion (manubrium) VS upper posterior ribcage expansion (T2-T4)?
Answer: The thing with expansion anywhere is that it’s not on/off switches with exercises. You can get expansion with a variety of moves and positions.
If we want to bias expansion into the manubrium (anterior T2-4), we have a few different options:
- High reaches (say 100°-180°) – because of circumferential expansion when going overhead
- Humeral extension – Due to scapular anterior tilt. And downward rotation biasing pec minor
- Cervical/Trunk Rotation – Due to general anteroposterior expansion that accompanies rotation
- Inversion – Due to gravity assisting the lungs in filling top-down
Some of my favorite activities to make this happen have been listed above.
I didn’t talk much about inversion, but my two money moves are the drunken turtle:
and decline quadruped on elbows:
If you want to progress to something a bit more challenging after doing these moves, I would check out this post on all things push press.
Sum Up
- Scapulohumeral rhythm involves combined posterior and anterior expansion, with the overall tendency occurring toward scapular AND humeral external rotation.
- An anteroinferior humeral glide during flexion (barring injury) occurs due to eccentric bias of the inferior humeral tissues.
- Specific limitations in thoracic expansion can be addressed by corresponding shoulder flexion loss with other measures.
- Manubrial expansion (T2-T4) occurs by using high reaches, humeral extension, cervical/trunk rotation, and inversion.
Image by Taco Fleur from Pixabay