Case studies are much more valuable than many give credit for.
It is this type of study that can often lead to sweeping changes in how further research is conducted, often create paradigm shifts in their own right.
After all, there was only one Patient H.M.
One thing that I wish I saw more in case studies was the clinician’s thought process. Why did they elect to do this treatment over that, what were they thinking when they saw this? How do they tick?
I was fortunate enough to have an online client of mine suggest to that I make her a case study, and it was a very rewarding experience on both fronts.
My hope is that you can see how a clinician thinks first-hand, and see the challenges a clinician faces…
When you can’t work with your hands.
Table of Contents
The Problem of Sitting – Her Story
This woman has been through some shit.
Valerie is a young physician who works quite a bit on her computer, helping many patients who are in dire straights and life-threatening scenarios.
Approximately three years ago, she developed a right frozen shoulder out of the blue, which seemed to resolve with injections and a few physical therapy sessions.
Just when she thought she was in the clear, Valerie developed right wrist and shoulder pain on the same side about one year ago. She attributed this development to a poor ergonomic set up at her office. Imaging for this problem was negative.
Despite making relevant ergonomic adjustments, she still had pain.
Valerie went through all the conservative measures that you’d normally go through for this problem. Six months after her initial pain development, she tried round 1 of physical therapy. This therapist focused predominantly on neck manipulation, which did provide some relief.
What didn’t provide relief, in fact worsened her symptoms, was a lumbar roll. This strategy was encouraged by the clinician to attain a better posture. Once she started sitting with the lumbar roll, her symptoms got worse and began to spread to her upper back.
Later, Valerie was referred to another PT who focused on scapulothoracic strengthening exercises. This clinician told Valerie that her lower trapezius muscles were extremely weak, and this contributed to her pain experience.
This rehab phase was quite difficult for her. Valerie had a very hard time finding and feeling these areas working. With time, she was able to get her left side to fairly strong.
All was hunky dory until Valerie attempted the prone Y exercise, a classic PT move.

Once she started working this movement, Valerie began to develop pain underneath her right armpit and along the right side of her trunk.
During this time she has also been seeing a trigger point therapist three times per week with some relief.
She emailed me because her physical therapy options were exhausted, and thought my online movement consultation would be of help. She did her research on breathing, PRI, and protective strategies, so she knew her stuff.
My Initial Thoughts
Though I still feel the subjective is more about developing a therapeutic relationship with the client and ruling out potential red flags, you can still glean some potential insights regarding your treatment strategy.
Two big things stood out to me:
- Lumbar extension from the lumbar roll making her symptoms worse
- The prone Y exercise making her symptoms worse
I’m generally not a big fan of either of these strategies. Most of our clients utilize extension-based postures and positions as a normal strategy. Extension increases when undergoing a stressor, much like our heart rate increases. Extending reduces mobility in all three planes to afford better body control, since fewer degrees of freedom must be accounted for.
There is a reason why extension is the closed packed position of almost every joint in the body.
Sitting for prolonged periods is a stressor. Even if ergonomic setup is great, staring at screens for multiple hours is evolutionarily new for us to cope with. Intense focus at a screen can be demanding from a postural standpoint, so to be most efficient, it would make sense to drive extensor tone to increase efficiency in sitting and focus.
However, limited mobility and joint position can create tissue ischemia. This is why your butt gets sore after sitting for too long.
So what happens when I drive further extension via a lumbar roll or a prone Y in someone who is already in extension?
Prollems, son. Prollems.
These strategies likely further created an ischemic response, leading to new pains developing in new areas. Someone with persistent pain can also develop larger receptive fields for nociceptors, which could be a potential explanation for some of the spreading pain that Valerie was experiencing.
You can already tell we need to get this woman out of extension. The question is how.
Focus on Sagittal Plane Control – Session 1
Subjective
Most of the subjective history was taken via email so we could spend more time on the evaluation and treatment side of things. But I did gain a few new insights:
- Valerie notices she leans on her right hip a lot
- Sitting “Indian style” is limited on the right
- Sleeping only 5-6 hours per night
We then discussed what particular movements make her worse.
Aggravating Factors:
- Any computer or phone work
- Mousing after 20-30 minutes
And then what helped her out.
Relieving Factors:
- Ice and heat
- rest
Here wear some other relevant things from a medical history standpoint:
- Acid reflux diseaseFor exercise, Valerie preferred walking or the elliptical. Any activity that involves impact bother her knees.
Her goals, aside from working without pain, was to have a more intensive exercise program. She wants to be able to do pushups and chin-ups #luv.
My Thoughts
Many of these findings—limited right hip external rotation, right hip leaning, and symptoms with right-handed mousing—corroborate with a normal right lateralized asymmetry we all have. These findings seem to mimic the left-sided extension/Zink/Left AIC/Right BC pattern inherent in many of us.
As the body extends joints on the left side, right side body demands increase because 1) there are more degrees of freedom to utilize and 2) the larger right diaphragm makes it easier for us to breathe.
If I can’t offload the right side because of an inability to express frontal and transverse plane movement on the left side, could that contribute to some of the ischemic pains she experiences with prolonged postures?
I don’t think that the history of acid reflux disease is an incidental finding. GERD is often associated with concomitant thoracic pain, and an indicated treatment is elevating the head of the bed1,2. This position incorporates some cervicothoracic flexion, which likely opens the airway a bit more favorably and helps take the individual out of an extended position.
Let’s now look at her objective findings.
Objective
| Standing Reach Test | palms floor |
| Functional Squat test | 5/5 |
| Multi-segmental Rotation [MSR] (Left/Right) | 75%/50% |
| Rib angle | 70 degrees |
| Seated Trunk Rotation (L/R) | 50% bilaterally |
| Hip Internal Rotation (L/R) | 50 degrees bilaterally |
| Hip External Rotation (L/R) (used seated FABERS) | 90/60 |
| Active Straight Leg Raise [ASLR] (L/R) | 100 degrees / 90 degrees |
| Supine Shoulder Flexion (L/R) | 180 degrees bilaterally |
| Supine Shoulder External Rotation (L/R) | 90 degrees bilaterally |
| Supine Shoulder Internal Rotation (L/R) | 40 degrees / 30 degrees |
| Active Midstance Test [AMT] (L/R) | 5/5; 0/5 (can’t achieve position) |
| Active Hip Abduction (L/R) | Normal bilaterally |
| Shoulder-Specific Tests | Standing Left shoulder flexion limited Pain with Right shoulder abduction |
My Thoughts
Obviously, evaluating virtually is a bit more challenging than in-person, so I’ve had to find tests that give me as much possible data on her triplanar movement capabilities.
The only real comparable sign that I had for her that was meaningful to Valerie pain-wise was shoulder abduction. We used this to make sure we were heading in the right direction.
As for relevant tests, consider the following from an upper body standpoint
- Asymmetrical standing MSR
- Limited seated trunk rotation bilaterally
- Limited shoulder internal rotation bilaterally
Here we see limited transverse plane activity in both the thorax and shoulders. Consider that the thoracic spine’s closed packed position is extension. If I extend at this joint, my inability to rotate ensues. Seeing her side profile you could see that her thoracic spine was flat.
If the t-spine is flat, then we develop what I call the “square peg in round hole syndrome” at the scapula. Since the scapula is a concave surface, it needs a convex surface along the ribs to have ideal bony congruency.
What happens if my thoracic spine is in extension? Well, the ribs in the front externally rotate to cause a rib flare, which causes the back-side of the ribs to migrate forward, reducing their normal curvature. This flattens the convexity needed for the scapula, creating the aforementioned syndrome.
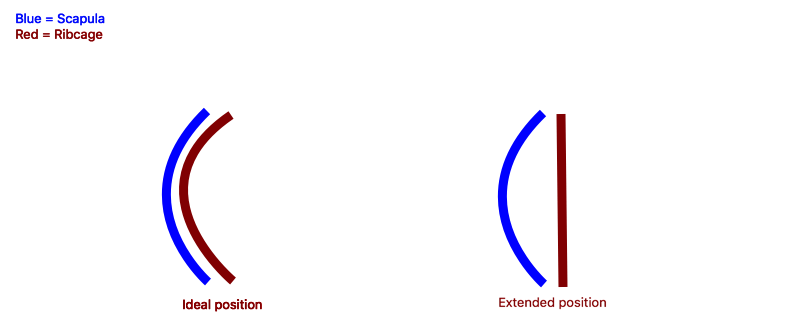
Since the scapula craves convexity, oftentimes it will migrate forward into a state of protraction, since better semblance of convexity can be established at the lateral aspect of the ribcage. As the scapula migrates forward, the glenohumeral joint follows along for the ride.
As I pull the shoulder back to test internal rotation along the surface of the floor, the glenohumeral joint has to glide anteriorly. Guess what that joint’s closed packed position is?
Abduction and external rotation, which is precisely where I am putting the joint during supine internal rotation. This positioning is likely a contributing factor to why she is limited when we test internal rotation.
Let’s now consider the lower body tests:
- Palms the floor on standing reach test
- Hypermobility of standing reach test and asymmetrical ASLR
- Full functional squat
- Large amounts of hip rotation
- Asymmetrical AMT
These tests tell me that Valerie is a flexible chick. Ability to squat, touch toes, asymmetrically large ASLR, and cray cray hip rotation indicate possible hypermobility.
With great mobility comes great responsibility.
The limited active mid stance test indicates that Valerie has a hard time with basic lumbopelvic motor control. The combination of hyper mobility without basic motor control = need to protect = pain.
You guys probably haven’t heard of the AMT. This test spurned out of necessity after a conversation with Daddy-O Bill Hartman. He was telling us about testing one’s active ability to adduct the hip against gravity. So kudos to him for this one.
I’m actually now using this test along with the Copenhagen Adductor exercise exclusively instead of the Hruska Adduction lift test, and here is why I like this combination better.
- Both feet are in contact with the ground at all times, which gives a better appreciation for functional coordination of hip musculature with ground contact
- The hips are in a position that better mimics mid-stance
- There are fewer potential compensations and it’s easier to appreciate those compensations when you can take a 360 degree view
- The Copenhagen adductor exercise is evidenced-based³, and allows me to test capacity/fatigability of relevant lumbopelvic musculature
Here’s how to do the AMT
Set-up (test side is named for top leg)
- Client is in side lying
- Top-side hip is placed in 90 degrees hip flexion, with the knee contacting the ground
- Bottom-side hip is placed in 0 degrees hip flexion, with knee contacting the ground
- Hips are slightly tucked via a posterior pelvic tilt without allowing the bottom leg to fall into hip flexion
- The top arm is placed on the ground in front of the abdominal region to allow for support.
Performance
- Flatten both feet on the ground, so bottom-leg heel and top-leg arch are in contact with the ground.
- Slide the top knee slightly forward and up while keeping arch contact with the floor. You should feel your top-side glute contracting.
- Maintaining body position, lift the bottom knee up while keeping the bottom heel contacting the floor. You should feel the bottom inner thigh and outside hip (gluteus medius, not tensor fascia lata) contracting. Do not allow the top knee to shift backward.
Here is how I score the test:
0 – Cannot achieve starting position (i.e. cannot place the bottom-side hip to 0 degrees flexion)
1 – Can achieve starting position, but cannot flatten both feet on the ground
2 – Can keep feet flat on the ground, but cannot lift the top knee off the ground or cannot feel top-side glute working (may compensate with top-side adductor)
3 – Can lift top knee off the ground and feel top-side glute (without top-side adductor) working, but cannot lift the bottom knee off the ground while feeling inner thigh and outside hip (may compensate with TFL or shift right knee backward)
4 – Can lift both knees off the ground, but only feels either inner thigh or outside hip working
4- indicates inner thigh, no outside hip
4+ indicates outside hip, no inner thigh
5 – Client can lift both knees off the ground and feel all relevant musculature working
Valerie was a rock-solid 5 on her left side, but could not place her hip into 0 degrees extension on her right. This gave her a 0. Inability to achieve full hip extension indicates increased hip flexor activity, a tell-tale sign that she favors extension.
Treatment
I gave Valerie two exercises to start, with the goal being to establish sagittal plane motor control.
Exercise 1 – Quadruped on elbows right glute max
I chose this activity because the quadruped position is a great way to establish a zone of apposition (ZOA), facilitate abdominal activation and breathing against gravity, and introduce spinal flexion. Having her upper back not contacting the ground allows for her to flex her thoracic spine every time she inhales while the abs hold the ribcage in a dropped position.
I typically perform this activity in quadruped, but when we attempted the exercise with her hands contacting the ground, she couldn’t relax her neck muscles. This compensation indicates that she is using accessory musculature to both stabilize in this position and breathe—a no-no.
Having her drop down to her forearms shortened the lever arm for her to support herself, and allowed her neck muscles to relax. Her goal was to work toward hands and knees without her neck kicking in.
As for the lower body offset position, this shift is intended to offload her favored right side. Adding the knee press into the wall allows us to improve hip external rotation by contracting her gluteus maximus.
Result
- Right AMT improved to 3/5
- Shoulder internal rotation improved to 60 degrees bilaterally
- No change in shoulder abduction symptoms
These results demonstrated we were able to reduce extensor tone enough to improve some rotational mobility at the thorax, and the change in the AMT indicated improved sagittal plane control.
Being able to flatten the feet indicated that we didn’t need to stretch out her bottom-side hip, but inability to lift the bottom leg demonstrated we eventually needed some frontal plane action.
I was not happy that we didn’t get any symptom relief, so based on her having symptoms on the right lat-region, I gave her this next activity for symptom management and to reinforce ZOA.
Exercise 2 – Right Doorway Lat Stretch
For some reason, internally rotating the humerus seems to give a better stretch than not.
Result
- Reported no pain with shoulder abduction
My Thoughts
I’d say a good first session, but we likely know she will need more frontal plane work by the next time we work together. I dosed the activities at 3-5 sets of 5 breaths, 1-2 times per day. This amount is typically enough volume to elicit changes in the two-week time period we’d have between sessions.
Building the Frontal Plane – Session 2
This session occurred two weeks after our first session.
Subjective
After about one week, Valerie was able to switch to hands and knees for the right glute max activity, and overall was doing pretty well. She reported reduced upper back and wrist symptoms, while feeling improved trunk mobility.
In terms of functional improvements, Valerie was now able to perform computer work for 1-2 hours before symptom onset, and also noticed that her knees have stopped locking. This knee complaint is the main reason why she wasn’t running.
She was performing her home program for 2 sets of 5 breaths twice a day.
My Thoughts
It seemed as though we were on the right track given the positive changes. Likely increased thorax mobility could be reducing the ischemic response she gets from prolonged computer work. If both shoulder and neck mobility improved, this may contribute to reduced strain at her wrist, given the links between neck position and grip strength4.
The knee unlocking thing was an interesting phenomenon. It’s possible that the locking sensation was merely Valerie struggling to shut off her quads while performing higher intensity activities. Given the limitations in hip extension she initially had, overactive quads could’ve increased extension at the knee joints, creating the “locking” sensation.
Objective
| MSR (L/R) | 90/75 |
| Hip External Rotation (L/R) (used seated FABERS) | 90/75 |
| ASLR (L/R) | 90/90 |
| Supine shoulder internal rotation (L/R) | 65/60 |
| AMT (L/R) | 5/5 / 2/5 (felt right adductor) |
| Active hip abduction (L/R) | -/+ (felt right adductor, not gluteus medius) |
| Shoulder | Pain with Right abduction; L HG FLEX full |
Objectively I cut down the testing to the limited ones. This allowed for more time to focus on progressing Valerie’s exercises.
As we can see, we got some favorable changes in our measures. We have closer to symmetrical hip external rotation, and the symmetrical ASLRs indicate we got enough sagittal plane control.
I liked seeing the MSR and shoulder IR improve as well, indicating we were on the right track from a thorax mobility standpoint.
Seeking to improve the AMT drove a lot of my next exercise selection. Obviously she now had requisite frontal plane mobility, but lacked control in this plane. This was corroborated with the worsening of the active hip abduction test. Now that we had frontal plane mobility, the right adductor was kicking in to enhance stability.
Due to reduced hip frontal plane motor control, improved thorax mobility, and continual symptoms with frontal plane shoulder movements, I wanted to emphasize straight frontal plane pelvis and thorax to see where that would take us. Frontal plane is typically the next target if sagittal is mastered.
Here was my exercise selection.
Exercise 1 – Left Sidelying Foot Toward Ceiling with Right Glute Max and Right Apical Expansion
Phew, how’s that for a name right?
I chose this activity to address a multitude of factors. Lifting the bottom leg in straight hip adduction would give me a frontal plane in the mid-stance position, while driving the right hip external rotation may gain her some more hip external rotation while inhibiting the right adductor.
The right arm going overhead would provide an active progression from the passive lat stretch we gave her last time, hopefully improving thorax mobility in the process.
Result
- Right AMT 4-/5 (could not feel gluteus medius)
- improved right hip abduction, though still could feel adductor
A nice change, but I wasn’t satisfied. We needed another way to inhibit the right adductor while simultaneously getting her to feel her glute med contract. Continual reliance on the right adductor for stability will make offloading her right side challenging.
We needed to give her a left inner thigh combined with a left outside hip as an alternative option for stability.
I had just the thing:
Exercise 2 – Left Sidelying Left Flexed FA Adduction with Right Extended FA Abduction and Left Abdominal Co-Activation
Aka lady in glasses on a milk crate
With the top leg abducted, we could better directly inhibit the right adductor using a purely frontal plane maneuver. Flexing the bottom hip allowed for Valerie to feel her left gluteus medius contract, as the lever arm for that leg was shorter.
Result
- Right AMT 5/5
- Normal active right hip abduction
- Shoulder internal rotation 70 degrees bilaterally
- No pain with shoulder abduction
We have a winner! These two activities were her home program.
Despite her symptoms being predominantly upper body, I elected to go with relatively lower body-heavy movements. She needs a sturdy base of support under a more mobile thorax, otherwise she will continue to extend. Increasing lower body motor control while simultaneously improving thorax mobility meets this need.
Valerie was pretty smoked from these two activities, so I told her to work up to 5 sets of 5 breaths for each if possible to increase capacity. We will meet again in two weeks.
Put it All Together in Standing – Session 3
This session occurred two weeks from session 2, totally 6 weeks for treatment.
Subjective
Valerie had exciting news to report. She no longer feels any right sided symptoms, and is not limited with her computer work. She wants to now fill in the rest of the pieces so she is good to go!
She did mention she occasionally gets right-sided foot pain and was wondering if she needed orthotics. She did buy a good pair of shoes to try and help with this.
My Thoughts
Very pleased with the progress thus far. I wanted to give her some standing activities that would further challenge her ability to coordinate the skills we had worked on for the last two sessions. At this point, I aimed to encourage Valerie to start up a fitness program of sorts to build intensity, as this would be beneficial for her long term health.
Objective
| MSR | 90/90 |
| Hip External Rotation (L/R) (used seated FABERS) | 90/80 |
| Supine shoulder internal rotation (L/R) | 80/80 |
| AMT (L/R) | 5/5 / 2/5 |
| Active Hip Abduction (L/R) | Normal bilaterally |
| Copenhagen adduction (L/R) – named for top leg | 2 reps/ 1 rep |
| Shoulder | No pain with shoulder abduction |
Here is the Copenhagen adduction test for those unfamiliar
Really pleased with the changes in thorax and hip mobility. Her right adductor still needs to be quieted down, but the fact that she can actively abduct the leg without it kicking in is a good sign.
Two key findings substantially influenced where we were going with Valerie next:
- Valerie’s ability to perform the Copenhagen despite the adductor hyperactivity in the AMT
- Occasional right foot pain
These factors led me to hypothesize that Valerie wasn’t getting adequate sensory input from the ground to inhibit her right adductor. I hate going down these rabbit holes, so the less outside help we need to seek the better.
What I first had Valerie do before we did anything was put her shoes on, walk around, and retest the AMT.
Result
- Right AMT (with shoes on) = 5/5
Bingo. That gave me the information I needed. Manipulating the footwear alone demonstrated that she had the motor skill necessary to perform the task, she just needed better floor awareness to use it. Also, because we were able to positively affect the tests without orthotics, I told her those would not be necessary at this time.
We needed to give her a challenging standing task to make these work. I chose two activities, one that emphasized left stance to offload her right side, and another to work on simultaneously sensing her right glute with her right arch to inhibit the adductor in standing
Exercise 1 – Left Lunge Medium Guard
This activity emphasized left stance to offload the right side and thoracic flexion. We initially tried the high guard position for this (see below), but she was complaining of some pain in the upper trapezius region. This compensation likely indicated she was extending during this task. Going with medium guard ensured she was staying in a more flexed position.
She could only do two sets of 5 breaths before fatiguing.
Exercise 2 – Right Lunge High Guard
This activity worked on the floor-hip connection I mentioned previously. She was able to sustain the high guard position, which got us that right lower trap that was weak per her last therapist.
Came full circle didn’t we?
Again, like the left lunge, she could only do two sets before fatiguing.
Result
- Copenhagen – able to perform 3 reps bilaterally.
I was super happy with how well Valerie did with these maneuvers, and the fast fatigability indicated she could continue to derive benefits from these strategies. I told her at this point that she would benefit from building fitness, and if she so desired we could eventually build her up to a running program.
Post-Treatment Clinical Reflections
If there is one thing you noticed, it’s how I used objective testing to guide my treatments. Symptoms, especially those sustained for prolonged periods, can oftentimes vary and be unreliable.
Having a system that aims to progressively restore triplanar mobility and motor control can allow an individual enough movement variability to reduce pain and go on to building fitness.
Fitness is the ultimate goal given all the health benefits. Increased fitness allows for better tolerance to life’s stressors, and in Valerie’s case, offsets the deleterious effects of prolonged sitting. I wish that I would’ve emphasized this more earlier on while working with her.
Her case also made me think a lot about my orthotic use, which is now considerably reduced. I use the term orthotic to encompass all types—shoe, dental, glasses, etc.
Valerie had asked me if we needed to go the orthotic route, including vision and dental, to get “fully neutral.” I now question how relevant this really is.
I think the quest for neutrality, full variability, whatever you want to call it, is a matter of degree. How far down a path we have to go is entirely idiosyncratic. Any intervention ought to be based entirely on what that person’s goals are, and to what extent movement variability is the rate limiting step. In many cases it’s less than you think. In even more cases, the basics were not fully mastered before going the orthotic route.
My company line as of today is to get enough mobility and motor control to get people out of pain and to allow them to perform all their desired physical tasks.
The farthest I now typically go with most people in terms of orthotic use is footwear and shoe orthotics. These tools seem to be the most impactful, and are a bit more evidenced based than dental and visual orthotics.
Yes, I say this after having going the dental and visual route myself. After spending time working with these orthotics, getting my wisdom teeth extracted, and getting my nasal airway surgically opened up, I can confidently say I am still far from neutral. Shoulder internal rotation just isn’t happening.
And I’m totally cool with that.
That said, I’m not trying to discredit that these devices do work for some people, or there are cases in which they are warranted. If someone has sleep apnea or a visual disorder, you bet I’m calling a dentist and optometrist. For me personally, I was able to fully squat and pistol squat within two weeks of getting my splint and glasses. For the first time in my life!

My client use with orthotics thus far has been a crapshoot. They do something, but we just don’t know what and for whom. Nor do we have much evidence to back up their utilization.
I think there are other low hanging fruits to go after that are much better researched, and likely more systemically effective. Dialing in nutrition, exercising, regular physical activity, stress management, and sleep hygiene are all areas that can have profoundly favorable systemic changes, reduce pain, and mitigate inflammation.
And they all have the research to back it.
Does it make sense to go for glasses if your client is 100 pounds overweight, eating twinkles on the regular, hasn’t exercised since the Nixon administration, and works as a stockbroker in New York City? I think we have to re-prioritize where we intervene on clients, and a multi-modal, health-focused approach is the way to do so.
But enough of my ramblings, here’s what Valerie had to say:
Valerie’s Testimonial
Over the course of one year, I developed severe upper back, lower back, and right shoulder pain. It was Unresponsive to traditional measures such as pain medications or topical agents. The pain was significantly affecting my quality-of-life. I was cranky and miserable around my family. I even thought about possibly even giving up my career ( which took over 10 years of education to achieve) because it is very computer intensive and the keyboarding/mouse work was nearly unbearable. I would become depressed just looking at my workstation.
In short, I was a miserable total mess. Initially, I went to physical therapists closer to my home, performing an extensive amount of rehabilitation exercises which took up one or two hours each day. It was so frustrating because I was diligently performing the exercises, yet I was not getting better, in fact some symptoms were getting worse.
Through extensive online research and the all important Dr. Google, I discovered Zac and scheduled an online consultation. He performed a detailed evaluation, looking at my entire body ( something no one else had done) and movement mechanisms. He Prescribed two exercises, much simpler schedule than previous regimens. Within about 10 days, I began feeling so much better. My back began to open up and my shoulder felt much better.
Now, after three sessions, I am able to work at my workstation completely pain-free, something I’ve been unable to achieve in one year. I’m getting a lot stronger physically and mentally. On another note, I feel like I’m a much better mother And wife now as well, the pain took up such a large amount of my energy.
Thank you Zac for helping me get my life back on track!
-Valerie R, Houston, TX
Sum Up
I hope you guys found seeing into my thought process informative, and I’d say this is often the general framework that I operate under with many clients.
To summarize, here are the big clinical pearls:
- Master sagittal, build frontal, touch transverse, then coordinate them all together
- Give the thorax a stable base to move from
- Motor skills must eventually be trained while contacting the ground
- A program should promote long term health
- Go after low hanging fruits and mastering the basics before trying advanced, experimental concepts
If you’d like to work with me online like Valerie, you can sign up at my services page.
I offer mentoring, movement consultations, and training.
What treatments do you incorporate for people with upper quadrant symptoms in sitting? Comment below and let us know.
References
1 – Komleva NE, Marjanovsky AA, Danilov AN, Agasarov LG. The novel approaches to the rehabilitation of the patients presenting with gastroesophageal reflux disease and co-morbid pathology. Voprosy kurortologii, fizioterapii i lechebnoi fizicheskoi kultury. 2017;94(2):20. doi:10.17116/kurort201794220-23.
2 – Huang HC, Fang SY. A systematic review of the literature related to elevating the head of the bed for patients with gastroesophageal reflux disease: applications in patients after esophageal cancer surgery. Hu Li Za Zhi. 2016. 63(6):83-93.
3 -Ishøi L, Sørensen CN, Kaae NM, Jørgensen LB, Hölmich P, Serner A. Large eccentric strength increase using the Copenhagen Adduction exercise in football: A randomized controlled trial. Scandinavian Journal of Medicine & Science in Sports. 2015;26(11):1334-1342. doi:10.1111/sms.12585.
4 -K. Grip Strength: Influence of Head-Neck Position in Normal Subjects. Journal of Neurology Research. 2012. doi:10.4021/jnr117w.
{kind=link}