
Table of Contents
So many shoulder measures, so little time. Where should you start?
If you have someone who has a mix of shoulder restrictions, you might wonder….
Eh, which one should I go after first?
This gets equally troublesome when few people have exactly the same restrictions.
What’s a fam to do??
You likely know how influential ribcage orientation can be, yet you can be laser-focused at which measures should be your target when you consider:
- Where each shoulder measure correlates to ribcage position
- Where to expand first pending infrasternal angle presentation
If you want to make your exercise selection much more accurate, this is the debrief, folks!
Check out Movement Debrief Episode 145 below to learn more!
Watch the video below for your viewing pleasure.
Or listen to my sultry voice on the podcast version:
If you want to watch these live, add me on Instagram.


Show notes
Check out Human Matrix promo video below:
Below are some testimonials for the class:
Want to sign up? Click on the following locations below:
February 20th-21st, 2021, Atlanta, GA (Early bird ends January 31st at 11:55 pm!)
April 10th-11th, 2021, Warren, OH (Early bird ends March 14th at 11:55 pm)
May 29th-30th, 2021 Boston, MA (Early bird ends April 25th at 11:55 pm!)
August 14th-15th, 2021, Ann Arbor, MI (Early bird ends July 18th at 11:55 pm!)
September 25th-26th, 2021, Wyckoff, NJ (Early bird ends August 22nd at 11:55 pm)
November 6th-7th, 2021, Charlotte, NC (Early bird ends October 3rd at 11:55 pm)
Dickinson College in Carlisle PA (POSTPONED DUE TO COVID-19) [Approved for 14 Category A CEUs for athletic trainers]
Montreal, Canada (POSTPONED DUE TO COVID-19) [6 CEUs approved for Athletic Therapists by CATA!]
Or check out this little teaser for Human Matrix home study. Best part is if you attend the live course you’ll get this bad boy for free! (Release date not known yet 🙁
Here is a signup for my newsletter to get nearly 5 hours and 50 pages of content, access to my free breathing and body mechanics course, a free acute:chronic workload calculator, basketball conditioning program, podcasts, and weekend learning goodies:
[yikes-mailchimp form=”1″ submit=”Get learning goodies and more”]
Motion of the shoulder complex during multiplanar humeral elevation – This is my go-to study when understanding scapulohumeral rhythm.
Elevate Sports Performance and Healthcare – The spot in Las Vegas where ya boi works.
Prioritizing shoulder restrictions
Question: If shoulder extension and horizontal abduction are both limited, which do you chase first? We could probably also add internal rotation in there.
Answer: Picture this, you have someone with measure XYZ limited on the right side, then ABC is limited on the other, where to start, fam?
If you’ve been following this site for a hot minute, you probably have the belief that humeral measures are used to approximate movement restrictions within the thorax. Put another way, airflow is going to be reduced in a given area based on particular shoulder measures.
Therefore, increasing shoulder mobility depends on where you have to put air and in what order you need to perform this.
When you are looking to improve shoulder measures, there are a few different principles that I operate by to enhance decision-making.
The lungs fill bottom-up
If you have a glass and you fill it with water, how does the water fill the cup?

The bottom-most parts of the cup fill first, then eventually it fills to the brim. You can’t fill the middle of the cup, then a little bit at the bottom, and a little bit at the top.
Your lungs are like that cup of water (that’s some philosophical sounding shit right?). When you take a breath of air in (assuming you are upright), the bottom parts of the lungs fill first, working up to the apex.
And just like that cup of water, you can’t expect to put a bit of air in the top, a smidge down low, etc.
You gotta fill those lungs bottom-up
Restriction in the thorax will generally lead to greater lung fill in the bottom portion of the lungs, with restricted ability to fill higher areas. Because the intercostals cannot expand the ribs, accessory breathing muscles will lift the ribcage as a unit, increasing bottom fill.
We want to restore the ribcage’s ability to expand in all directions. In order to make that happen, we have to restore this bottom-up fill that the lungs perform.
In order to know how to “fill” the thorax bottom-up, we have to understand how different shoulder measures can let us know where airflow is restricted.
The first heuristic that we operate from is breaking down how specific measures are related to thorax restrictions:
- Flexion, abduction, and external rotation restrictions indicate decreased posterior expansion
- Extension, adduction, and internal rotation restrictions indicate decreased anterior expansion
The reason why these measures are related is because of how scapular position changes when the thorax cannot fill adequately.
For example, if the anterior thorax cannot fill adequately, the shoulder blades will round forward, which leads to the humerus externally rotating to bring the arm back to center, causing an internal rotation loss.
Flip this for posterior restrictions, you’ll see a flatter upper back, which pulls the shoulders back, which leads the humeri to internally rotate back to center, causing an external rotation loss.
You can have a mix of in-between pending what thorax levels are restricted, hence the wide variety of postures people assume.
But how can you tell where the restrictions lie?
I’M GLAD YOU ASKED!
Each humeral measure corresponds to a different level of the thorax. It has to do with the fiber direction of tissue excursions you are testing and their location relative to spinal level. For example, the horizontal fibers of subscapularis run from around T2-4.
Let’s look at each of these measures and where they relate to on this fancy table. Only the finest for the fam!
Humeral Measures
| Test | Tissue Tested | Spinal Levels |
|---|---|---|
| Shoulder Flexion | All posterior thorax tissues | Entire posterior thorax with a slight bias towards T2-4 |
| Shoulder External Rotation | Oblique fibers of subscapularis | Posterior thorax at T6-8 |
| Shoulder Horizonal Abduction | Transverse fibers of subscapularis | Posterior thorax at T2-4 |
| Shoulder Extension | All anterior thorax tissues | Entire anterior thorax with a slight bias towards manubrium |
| Shoulder Internal Rotation | Oblique fibers of posterior cuff | Anterior thorax at sternal body (T6-8) |
| Shoulder Horizontal Adduction | Transverse fibers of posterior cuff | Anterior thorax at manubrium (T2-4) |
Or if you are more the graphic kind of person, peep this:
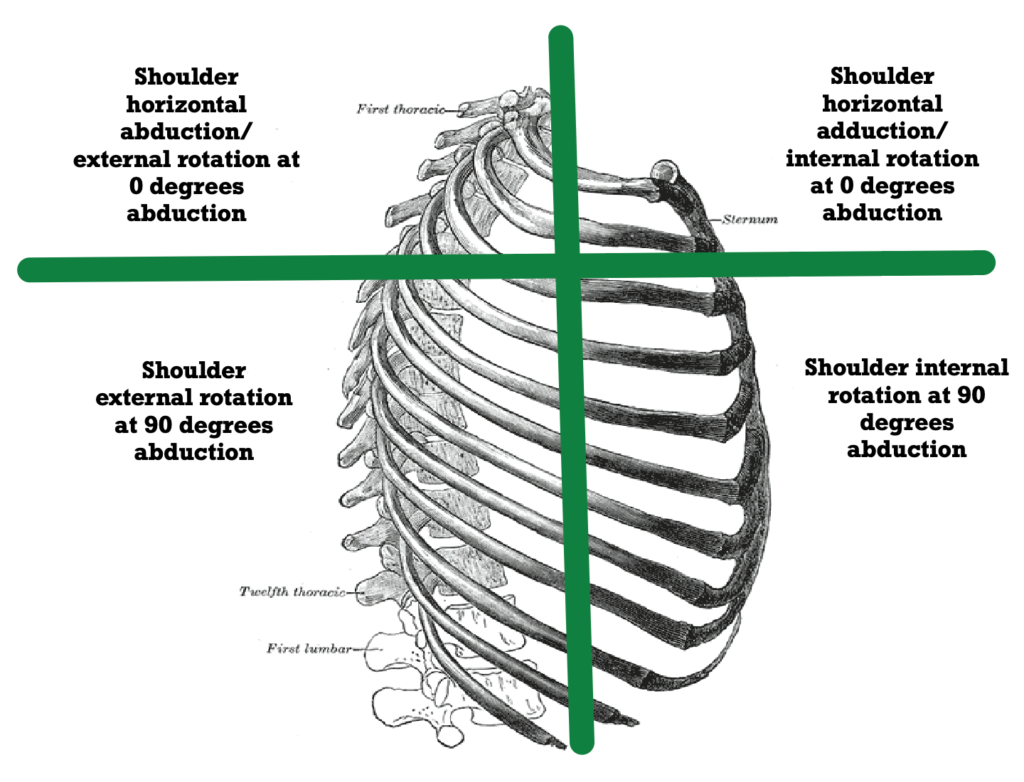
So for example, if someone has a loss of internal rotation and horizontal abduction, internal rotation would be the first priority because it’s a lower level on the thorax. of course, assuming you can stack, as that’s what fills up the thorax period.
Exercise options to improve thoracic expansion
Now that we know how to assess each level of the thorax, let’s look at some general ways of improving these measures.
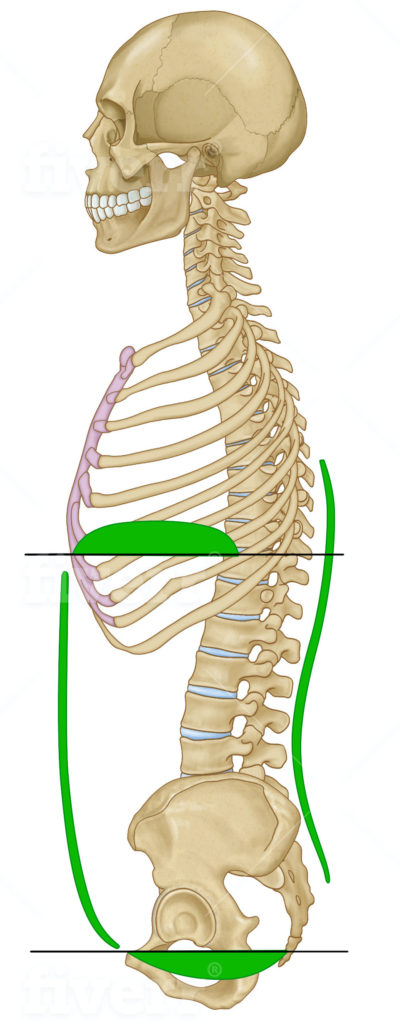
Before getting uber specific with each measure, the first priority is to coach the stack. The stack helps create the necessary piston effect between the thoracic and pelvic diaphragm to allow for the ribcage to expand in all directions.
If you lack the ability to stack (#bars), then there will be increased accessory muscle tone, the lower portions of the lung will receive the most fill, and you won’t have a whole lotta movement in your arms.
Now let’s suppose that you stacked (even though trust me, you probably didn’t), let’s look at some strategies for improving humeral measures:
- Shoulder external rotation: Reaching between 0°-60° shoulder flexion
- Shoulder internal rotation: Reaching between 60°-120° shoulder flexion
- Shoulder horizontal abduction: Drive thorax rotation while keeping the head forward, or drive active humeral external rotation. Driving cervical rotation
- Shoulder horizontal adduction: Drive humeral extension
- Shoulder flexion: Progressively go overhead, but restore external rotation and horizontal abduction first. You can also utilize rotation to make this happen
- Shoulder extension: Reach forward, then drive humeral extension
If you are in doubt, you can always drive rotation, which is an excellent way to drive anteroposterior expansion. You can also use inversion to get uppermost thorax expansion, as the lungs will fill top down in this case:
Now that we have an idea of what each measure means and what to do about it, how do I prioritize these restrictions based on the bottoms-up approach?
Simple (though not easy), you address the lowest most restrictions first, then work your way up:
- Achieve the stack (have the infrasternal angle be dynamic)
- Restore shoulder internal and external rotation
- Restore shoulder horizontal abduction and adduction
- Restore shoulder flexion and extension
How does the infrasternal angle impact order of addressing shoulder motion?
So we have an idea of where we need to put air, but how does the infrasternal impact the order of priority?
Different infrasternal angles and the accompanying skeletal structure predispose someone to predictable restrictions.
Based on the order that compensatory strategies occur with each archetype, you want to go after restrictions in the following order:
Wide infrasternal angle
- Dynamic infrasternal angle
- Address secondary compensations (limited extension, adduction, and internal rotation)
- Address primary compensations (limited flexion, abduction, and external rotation)
Based on the order of attack, as well as the filling bottom-up concept, you might approach the following wide ISA individual:
- Reduced shoulder internal rotation and horizontal abduction, and flexion
They would go after improving movement options in the following order:
- Dynamic ISA
- Shoulder internal rotation
- Shoulder horizontal abduction
- Shoulder flexion
Narrow infrasternal angle
- Dynamic infrasternal angle
- Address secondary compensations (limited flexion, abduction, and external rotation)
- Address primary compensations (limited extension, adduction, and internal rotation)
Based on the order of attack, as well as the filling bottom-up concept, you might approach the following narrow ISA individual:
- Reduced shoulder internal rotation and external rotation, horizontal abduction, and flexion
They would go after improving movement options in the following order:
- Dynamic ISA
- Shoulder external rotation
- Shoulder internal rotation
- Shoulder horizontal abduction
- Shoulder flexion
Sum up
- Shoulder restrictions correspond with airflow into the thorax at various levels
- Addressing restrictions should occur with a bottom-up approach
- The infrasternal angle and the order of compensation should be taken into consideration when exploring frontside or backside expansion first