Table of Contents
Got double chins for days and can’t open the neck up? Check this out
While there is no perfect static posture, it is not uncommon for someone who has a military head posture to have limited cervical extension.
Maybe you’ve tried a bunch of traditional moves to get it back, yet it still persists.
Oh, if only getting neck range of motion was so easy.
We have to ask in this specific presentation, why is cervical extension limited?
It turns out, there are three key areas that are interrelated AF that we need to hone in on to improve motion here we have to hone in on:
- Anterior thorax
- Hyoid
- Tongue
How are these three areas related to neck movement?
Check out Movement Debrief Episode 148 below to find out!
Watch the video below for your viewing pleasure.
Or listen to my sultry voice on the podcast version:
If you want to watch these live, add me on Instagram.

 t
tShow notes
Check out Human Matrix promo video below:
Below are some testimonials for the class:
Want to sign up? Click on the following locations below:
May 29th-30th, 2021 Boston, MA (Early bird ends April 25th at 11:55 pm!)
August 14th-15th, 2021, Ann Arbor, MI (Early bird ends July 18th at 11:55 pm!)
September 25th-26th, 2021, Wyckoff, NJ (Early bird ends August 22nd at 11:55 pm)
October 23rd-24th, Philadelphia, PA (Early bird ends September 26th at 11:55pm)
November 6th-7th, 2021, Charlotte, NC (Early bird ends October 3rd at 11:55 pm)
Montreal, Canada (POSTPONED DUE TO COVID-19) [6 CEUs approved for Athletic Therapists by CATA!]
Or check out this little teaser for Human Matrix home study. Best part is if you attend the live course you’ll get this bad boy for free! (Release date not known yet 🙁
Here is a signup for my newsletter to get nearly 5 hours and 50 pages of content, access to my free breathing and body mechanics course, a free acute:chronic workload calculator, basketball conditioning program, podcasts, and weekend learning goodies:
[yikes-mailchimp form=”1″ submit=”Get learning goodies and more”]
Bill Hartman – Daddy-O Pops himself. Originator of the hyoid position test.
American Academy of Orofacial Myofunctional Therapy – This is my go-to resource for all things myofunctional therapy. I did a course review of the one I attended.
Military head posture
Question: I’ve been enjoying the cervical extension test to help determine hyoid position. However, I had an issue last week where it didn’t work.
This client had a military posture. We did this assessment, but as they opened the mouth, they got no additional cervical extension at all.
Usually, additional cervical extension is expected with military neck posture.
The result threw me off, however, the person did have zero IR of the shoulder and I’m wondering if that had any influence on the cervical extension test.
Thanks, Homie!
Answer: The hyoid position test was created by Daddy-O Pops himself, Bill Hartman, as a way to assess hyoid position, which is essentially the infrasternal angle equivalent in the cervical spine.
In noncompensatory mechanics, the hyoid should be able to depress and elevate without restriction. Functionally, the hyoid normally elevates with swallowing, which you do like a BAZILLION times a day. Loss of dynamics in this area could impact swallowing, neck motion, and a whole lot more.
The hyoid position test is a way to assess the concentric bias of either supra or infrahyoid musculature.
If you notice a restriction within cervical extension, opening your mouth can oftentimes lead to an increase in motion by eccentrically orienting these frontside muscles, which has to happen as I tip the head back.
So then what should happen in the case of a military head posture?
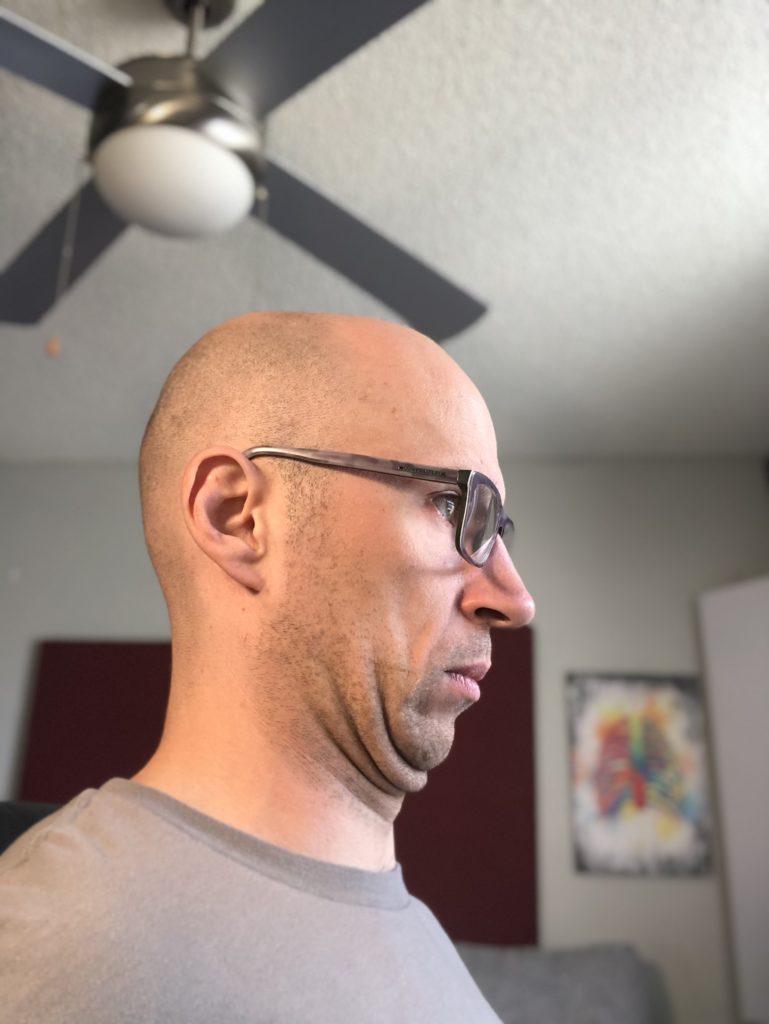
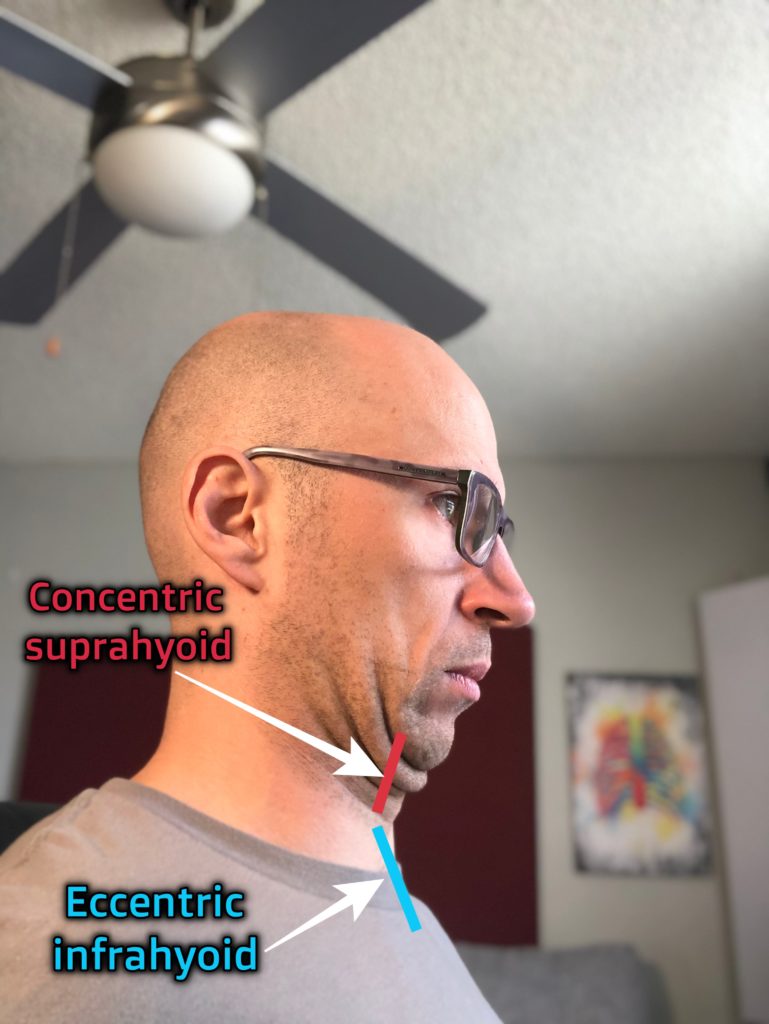
In this particular posture, the hyoid is elevated, which means that suprahyoid musculature is concentrically biased. You will also see lower cervical extension and upper cervical flexion.
Subsequentially, the infrahyoid musculature should be eccentrically biased.
In theory, when the mouth opens during this particular test, the upper cervical spine should tip further backward, enabling more range of motion.
But what happens when hyoid testing goes wrong?!?!
In the case that David mentions, we don’t see this happen. Why is that?
I’M GLAD YOU ASKED!
If the infrahyoid musculature is eccentrically oriented, the sternum should theoretically be in an “up” orientation. Anterior thorax expansion ought to be available, thus shoulder extension, adduction, and internal rotation should be free.
However, David’s tricky client doesn’t present in this fashion. If there is a shoulder internal rotation loss, then the infrahyoid musculature will be concentrically oriented.
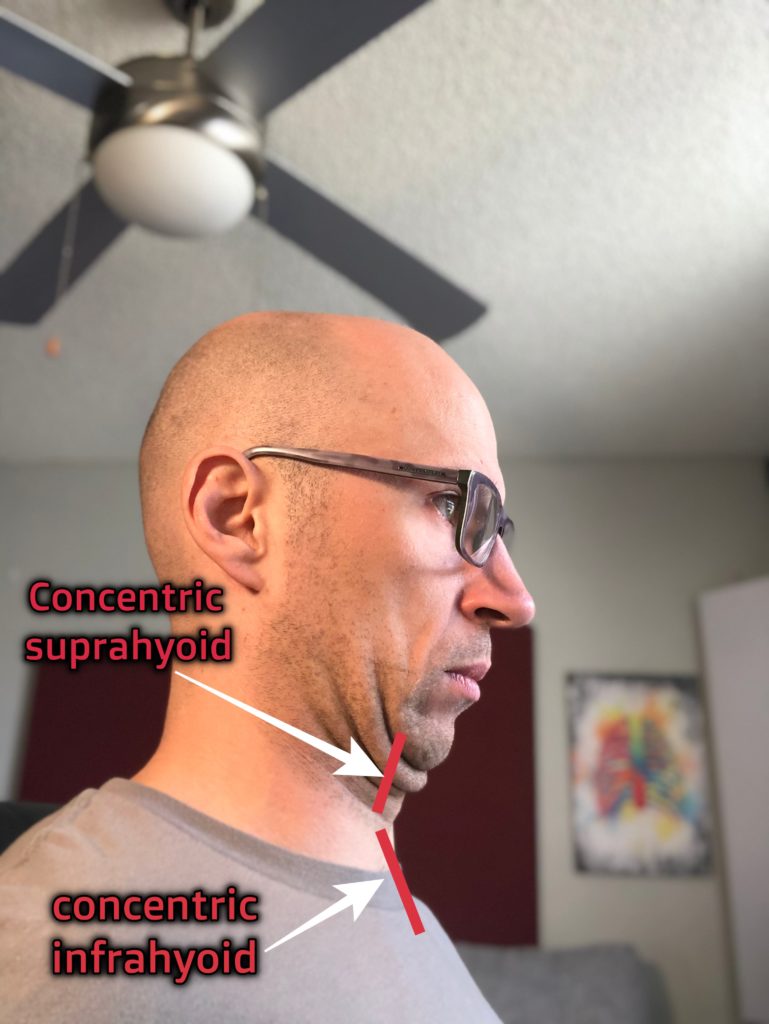
So what my boi David has is a double concentric. With this situation, there is no position that the hyoid can eccentrically move into, thus, no change in motion. You’ll likely either see restricted extension OR the thorax tilting posteriorly as the client extends, giving pseudo full extension.
What are you to do in this case?
The solution would be to create an eccentric orientation somewhere so you can induce some movement in the hyoid.
Following the filling the cup with water approach to airway dynamic restoration, you ought to start with getting the infrahyoid muscles to chill. This can be achieved by putting air into the front of that chest.
For a narrow infrasternal angle presentation, you may choose a quadruped activity, like the lazy bear.
For a wide infrasternal angle, you may reach about 110 degrees of shoulder flexion.
You then may have to drive manubrial expansion, which can be achieved with shoulder extension-based activities. Tricep extension exercises can work wonders here:
Okay, let’s suppose that your anterior thorax is now dynamic AF, how in the heck do you get the suprahyoid musculature to chill?
This process is twofold.
At the cervical spine, we have to drive OA extension without inducing a forward head posture. The cranium moves, not the neck

Simply cueing “undouble chin” during many moves can be helpful. You can kill two birds with one stone by choosing an activity where you are both driving air into the front of the chest and OA extension. A front plank can be a great choice:
Now I’ve played with the hyoid position test and altering dynamics in that area, but I think measuring what the tongue is doing might provide more information.
I want you to consider this. When we are measuring things like the infrasternal angle, proxy measures for the infrapubic angle, and the hyoid, what are we really looking at?
The answer, folks, is how well we can manage the internal anatomy:
- Viscera
- The airway
This issue with proxy measures is that we are looking at a proxy. An estimate. The further removed we are from the actual thing we are measuring, the more prone we are to inaccuracy with testing.
In my experience, the hyoid orientation is often prone to this, as many can achieve full cervical extension in a variety of compensatory ways. You may get some false negatives.
What if we could directly measure the internal anatomy that the hyoid test is looking at? It turns out, folks, we can. How can we do that you might ask?
The answer: The tongue
Tongue range of motion, posture, and dynamics are the rate-limiting step when it comes to hyoid orientation. Simply put, the hyoid cannot be dynamic if you cannot manage tongue placement.
Here are the factors that go into tongue management:
- Range of motion: Can you have roughly the same range of motion with a tongue tip open and a cave?
Here is what a “normal” amount of these measures looks like (I had a tongue tie release, so I cheated a bit):
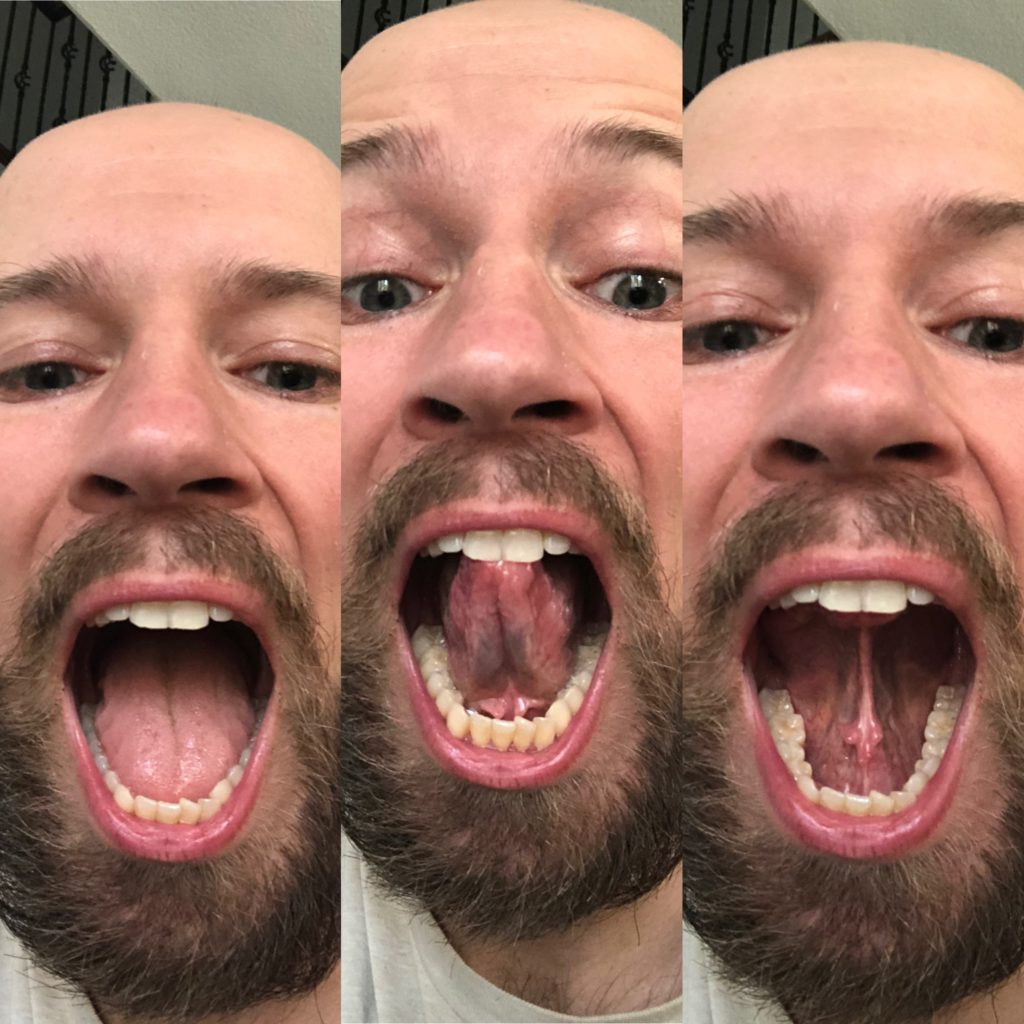
Compare that with the limitations noted in this client:

2. Posture: Can the tongue be fully placed on the roof of the mouth, lips closed, face relaxed, and breathe through the nose?
If the tongue sits low, it will encroach on the back of the throat, decreasing the space in the pharyngeal wall. This position will restrict the airway dimensions.
And get this shit, fam. OA flexion will cause the mandible to protrude more, which aids in opening the airway. Consequently, movement options will be reduced. Here, we see a compensatory strategy to keep the airway open.
3. Dynamics: Do you possess all the movement options the tongue should be able to perform?
There are TONS of different positions the tongue can assume, all requisites to practicing swallowing without compensatory strategies.
If you want to learn all the positions you need to practice, you can peep that here.
Sum up
- Military head posture involves lower cervical extension, upper cervical flexion, and concentric orientation of the suprahyoid musculature.
- If shoulder internal rotation is lost, the infrahyoid musculature will also be concentrically oriented.
- To restore movement options in this position, you must drive anterior thorax expansion, OA extension, and tongue position.
Photo credits: