
Table of Contents
If you have knee pain, this case study is a MUST to see
Does your knee cap point inward but your foot? point outward?
If so, then you MUST check out this post because we outline a critical factor with this postural presentation:
A “twisted” knee occurs for different reasons in different people.
I’ll illustrate why by checking out this narrow infrasternal angle case study below. You’ll find that the way this person does it is different from other folks.
Check it out below. Also, if you want to see the other case, you can find that here. (will be released on 6/26/2022)
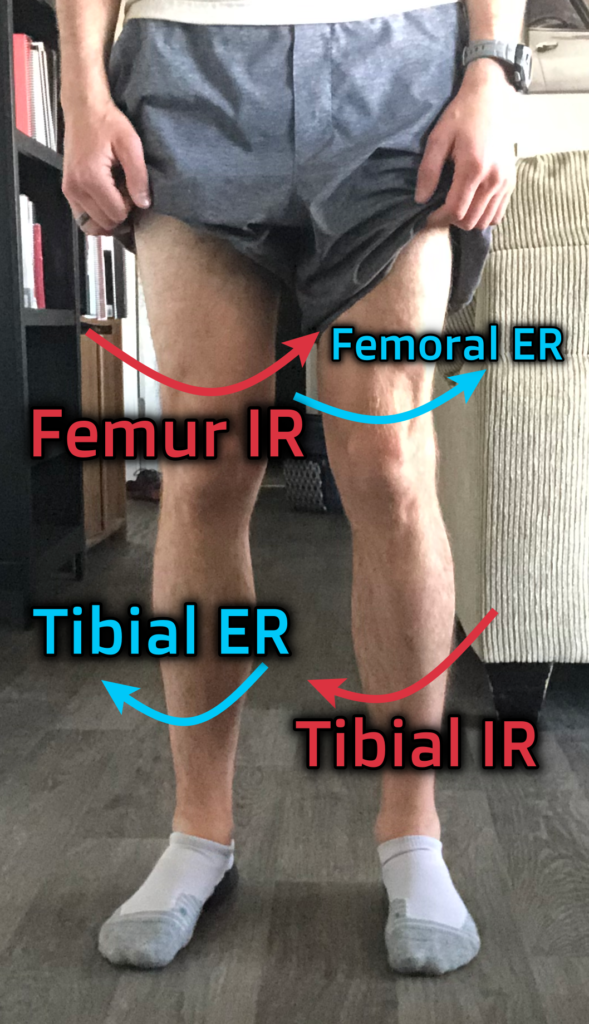
Why does the knee appear twisted?
Generally, A knee will appear twisted when you have the following combination:
- Femoral internal rotation
- Tibial external rotation
And it looks like this:
But here’s the deal, the components that create this twist occur differ among individuals. In fact, these are but a few of the factors that could contribute to the twist:
- Left hemipelvis anteriorly tilting
- Pelvis translating forward
- Pelvic rotation
- Distal femur ONLY internal rotation
- Tibial torsion
- Proximal tibial ONLY externally rotating
- Others I can’t think of off the top of my head
To illustrate how this can occur, we will look at two different cases, and how the “same” problem can require different solutions.
Narrow infrasternal angle with knee twist
So Jason is a friend in the fitness industry who sent me pictures of himself and one of his clients, wondering about the knee presentation in each of these cases.
Let’s first look at Jason so you can see what we are talking about.

As you can see above, it appears as though Jason’s kneecaps are a bit more centered/inward in comparison to where his tibia is. You can note this by comparing the tibial tuberosity location in relation to the knee cap position. Not a crazy amount of course.
We now have to ask how Jason is getting there. For that, we have to look at his measures. Jason gave me a few tests to look at.
Here’s his presentation:
| Test | Left | Right |
| Infrasternal angle (ISA) | Narrow | Narrow |
| Active Straight leg raise (ASLR) | 50º | 60º |
| Hip flexion | 100º | 95º |
| Toe touch | Above ankles, bends knees |
The above information is pretty classic of a narrow infrasternal angle presentation, and the asymmetrical ASLR likely indicates the beginning stages of a flat/longitudinal turn to the right on the pelvis.
You’ll also want to check out this pic here, which likely illustrates that
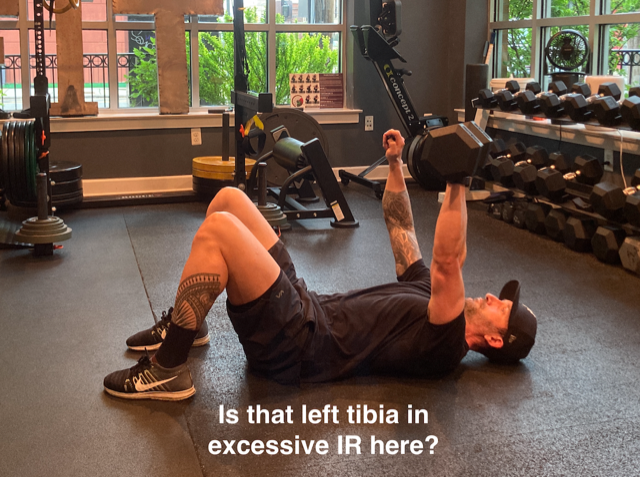
You can see how Jason is internally rotating the tibia a bit more on the left than the right (at least I think, it’s hard to tell at this angle, but he also pointed it out to me). As I progress in this turn, I’ll likely get more internal rotation occurring through the left lower extremity.
Although most of this turn is likely not occurring as much below the knee, hence why we see the twist. The reason why I say this is because of the foot posture that Jason exhibits.

Look at the space between his first and second toes. There’s a fairly large gap between them. This foot posture indicates a plantarflexed first ray, which accompanies calcaneal inversion. This action is exhibited in both early and late stance, which are external rotation representations. You can also see this with his higher arches. We are seeing a slight toe curl on the outer toes, which may indicate a more late stance representation.
Now Jason had mentioned that he used toe spacers, though I doubt this is the reason why we see this space since we don’t see similar spacing among the other toes.
So what do we do about it?
I’M GLAD YOU ASKED!!!!!
If Jason is in the flat turn, then we need to address that first and foremost, especially given the twist is mild.
FOr that, I’m currently using a 4-step sequence to address it:
- Stack
- Expand left posterior lower pelvis
- Left hip approximation
- Turn pelvis left from a right-oriented position.
Now you wouldn’t do all of these in one session, but I would be thinking of the following choices to help our boy out.
For the stack, I would use something like a quadruped exercise to start, not cueing much of a tuck:
To expand the left posterior lower pelvis, something like a short lever baby roll has been quite useful:
To get the left hip approximation, I use a standing version of this:
Lastly, turning the pelvis left, you can use a quadruped hip shift, which is absolute MONEY:
Now, if you do this and we still have some twisting action in the knees, then I think the half kneeling reach series is a go-to.
Here, the half-kneeling position promotes hip internal rotation (which a narrow ISA needs), then the pronation + external rotation action will help address the local knee mechanics needed to increase the available movement:
Sum up
Those would be the ways I would address this specific case.
To recap:
- A twisted knee occurs with femoral internal rotation and tibia external rotation
- If from a narrow presentation like this, we would stack, address flat turn compensations, and retwist the knee in the opposing directions.
What struggles have you had with knee problems? Comment below and let the fam know!