
Table of Contents
If your breathing is whack, learn these tricks from Zac
Coaching the breathing mechanics needed to improve movement options can be tough. Especially with all the various compensatory strategies.
These issues get even worse if you don’t fully grasp the mechanics.
Moreover, what if your supreme clientele think they have to be breathing this wild and crazy way 20,000 times per day?
We answer all these in more in today’s debrief.
If you feel like you haven’t maximized your ability to coach and apply breathing, this post is a must.
Check out Movement Debrief Episode 154 below to learn more!
Watch the video below for your viewing pleasure.
Or listen to my sultry voice on the podcast version:
If you want to watch these live, add me on Instagram.
Show notes
Check out Human Matrix promo video below:
Below are some testimonials for the class:
Want to sign up? Click on the following locations below:
August 14th-15th, 2021, Ann Arbor, MI (Early bird ends July 18th at 11:55 pm!)
September 25th-26th, 2021, Wyckoff, NJ (Early bird ends August 22nd at 11:55 pm)
October 23rd-24th, Philadelphia, PA (Early bird ends September 26th at 11:55pm)
November 6th-7th, 2021, Charlotte, NC (Early bird ends October 3rd at 11:55 pm)
November 20th-21st, 2021 – Colorado Springs, CO (Early bird ends October 22nd at 11:55 pm)
December 4th-5th, 2021 – Las Vegas, NV (Early bird ends November 5th at 11:55 pm)
Or check out this little teaser for Human Matrix home study. Best part is if you attend the live course you’ll get this bad boy for free! (Release date not known yet ?
Here is a signup for my newsletter to get nearly 5 hours and 50 pages of content, access to my free breathing and body mechanics course, a free acute:chronic workload calculator, basketball conditioning program, podcasts, and weekend learning goodies: Full Name Email AddressGet learning goodies and moreEdit Form | Customize Form
Prone hamstring curl troubleshooting
How the infrasternal angle affects diaphragm position
Question: Can you talk about crural/costal diaphragm fibers and their role as compensatory influence narrow and wide?
Answer: I thought a bunch after watching this video by Daddy-O Pops himself, Bill Hartman (he always makes me think and reflect dang it), and I concluded:
I was wrong.
I was wrong about the way the diaphragm is positioned in the narrow and wide infrasternal angle presentations. That’s because I was thinking about the diaphragm as only one muscle, that contracts as a unit.
In reality, muscles do not behave in this manner. In fact, according to this study, you can have selective recruitment in muscle fibers. Meaning, one portion of the muscle can contract more than another. Theoretically, I can have concentric orientation in one aspect of a muscle, but not in another.
A great example of this phenomenon is in the hamstrings after an ACL surgery. It’s not uncommon for peeps to have a loss of knee extension, yet have a CRAZY straight leg raise. How can this be?
Simple. The hamstrings would be eccentrically oriented proximally, and concentrically oriented distally.
So too could we have this in the diaphragm. Could it not be that one portion of the diaphragm have tension in it than another? I think so.
With this framework in mind, how would that look for each infrasternal angle presentation?
I’M GLAD YOU ASKED
To understand the diaphragm’s behavior, we must look at how the axial skeleton and lower ribcage is oriented in each.
First, the axial skeleton:
- Wide infrasternal angle: Increased lumbar lordosis (concentric/exhaled orientation)
- Narrow infrasternal angle: Decreased lumbar lordosis (eccentric/inhaled orientation)
If these orientations are present (exhaled for wide, inhaled for narrow), then the crural portion of the diaphragm (posterior) will present as follows:
- Wide infrasternal angle: Eccentric posterior/crural diaphragm
- Narrow infrasternal angle: Concentric posterior/crural diaphragm
Now let’s flip the script and look at the lower ribcage:
- Wide infrasternal angle: Inhaled lower ribcage (buckethandle up)
- Narrow infrasternal angle: Exhaled lower ribcage (buckethandle down)
If these orientations are present, then the costal (anterior) diaphragm is doing the following:
- Wide infrasternal angle: Concentric anterior/costal diaphragm
- Narrow infrasternal angle: Eccentric posterior/crural diaphragm
And the cool thing about this? The diaphragm orientations match the pelvic floor orientations for these infrasternal angle presentations.
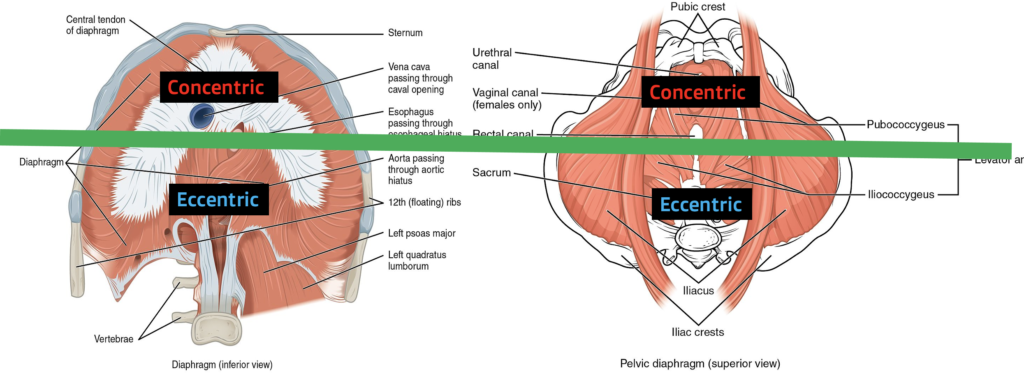
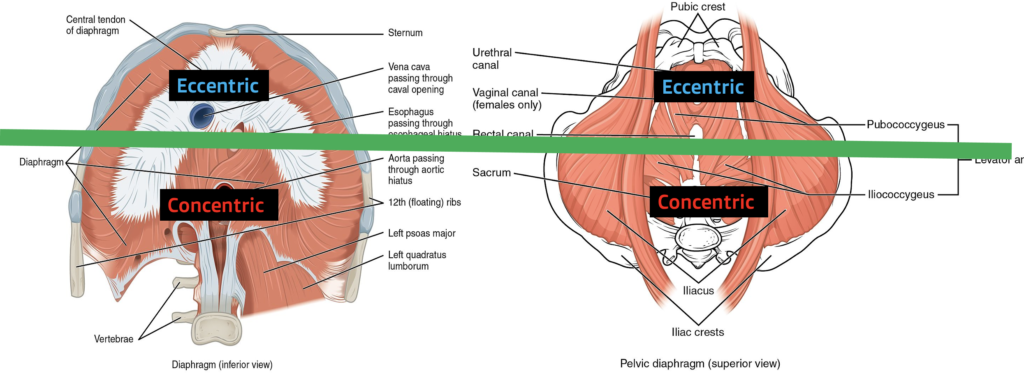
- Wide infrasternal angle: Concentric anterior pelvic floor/eccentric posterior pelvic floor
- Narrow infrasternal angle: Eccentric anterior pelvic floor/concentric posterior pelvic floor
Improving buckethandle dynamics
Question: What if your lower ribs don’t move upwards in inhale at first, at least not in bucket handle manner
Answer: “Normal” mechanics at the lower ribcage are as follows:
- Inhale: Ribs shoulder move laterally and superiorly (outward and upward)
- Exhale: Ribs should move medially and inferiorly (inward and downward)
We call this the buckethandle action of the ribcage.
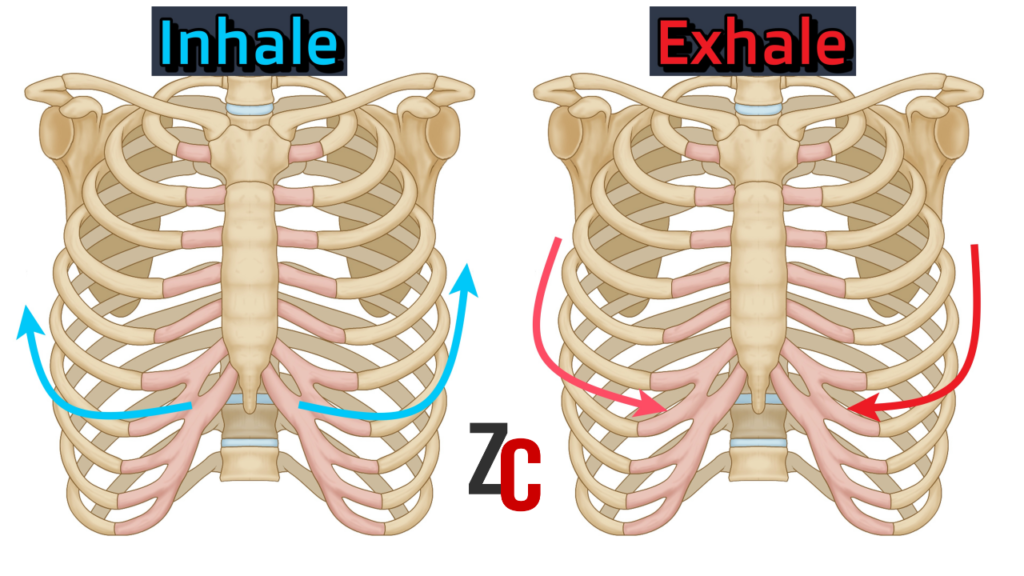
When you are working with those who aren’t well-versed in the dark arts, you’ll rarely see it. Most of your supreme clientele will have compensatory breathing strategies, with the ribs moving up and down, no lateral movement. This action occurs with concentric activity in the accessory muscles, and a subsequent loss of you being able to move your stuff everywhere.
Uh, we don’t want that fam!
In order to restore these mechanics, and get your body moving and grooving, you need two #majorkeys when it comes to coaching breathing:
- Exhale: Full and complete, with light ab tension created at the tail-end
- Inhale: Silent through the nose with minimal upper body tension; ab tension maintained
If you don’t have these components, then you won’t have buckethandle, and you won’t have a good time!
If we isolate this problem to a lack of buckethandle on the inhale, then the two issues you will likely be dealing with are:
- Loss of ab tension
- Using accessory muscles for inhalation
- Both
Therefore, you’ll want to have your supreme clientele focus on addressing these two areas.
If lack of ab tension is the issues, I’ll focus on cueing in the following manner:
- Develop awareness of ab tension at the end of the exhale (Have them palpate themselves to feel)
- Ask them to pause briefly while keeping the ab tension
- Ask them to keep the ab tension whilst inhalating (god I love the word whilst!)
If their neck looks like they are doing a max effort lift instead of inhaling, then I’ll usually have them proceed in the following manner:
- Have them palpate their neck to develop awareness of them creating all this dang tension
- Ask them to focus on breathing without creating that neck tension
- If the struggle is real, switch to nasal breathing only
If both of these strategies are an issue, then I would start focusing on getting the neck to chill, then get them to create the ab tension. If you hit it up in this manner, NO ONE will mess with you
How should I breathe at rest?
Question: At rest should I just breath away or is there a more precise way to do it though seems like you could drive yourself crazy as you analyze all 20,000 breaths is a day, hmm wonder who has done that.
Answer: It’s a common misconception to breathe the way I coach the stack during everyday activities. Wrong tool for the job big fam!
The stack breathing is used to increase available movement within the body. We are driving larger air excursions to increase movement options.
It’s unrealistic to do this breathing strategy during everyday activities. Walking is too fast, sport is even faster, and well, you won’t get any work done at your desk job if you are throwing a bazillion 5-second pauses between TPS reports.
But I get it, you want to be healthy AF throughout the day. Not do anything wild and crazy to mess up your stuff. Is there anything one can do?
Why yes my dear fam, there is!
What’s the “best” way to breathe throughout the day?
Nasally.
Nasal breathing has a ton of benefits over mouth breathing. It’s humidified and cleaner air, increases nitric oxide production (which dilates blood vessels), and a whole bunch of other stuff.
Movement-wise, mouth breathing can increase tension in accessory muscles, which limits movement options.
Uhh….WE DON’T WAN THAT FAM!
Therefore, if you are chillin’ like Bob Dylan, not talking to anyone, or even exercising, nasal breathing is definitely the way to go.
Here are the big keys to focus on to have your nasal breathing ON POINT:
- Mouth lightly closed
- Tongue completely on the roof of the mouth (with little neck tension)
- Teeth can either be contacting lightly or slightly apart
- Breathe quietly and easily through your nose

If this is a new thing for you, then you could try a few 30s bouts of breathing in this fashion, see how you do.
If you are struggle bus at this, you could have some issues in the upper airway that need to be addressed. If that’s you, I’d check out the following posts:
- Introduction to Orofacial Myofunctional Therapy
- Why I Had Tongue Tie Surgery at 32 Years Old
- Why I Am Expanding My Maxilla at 33 Years Old
- Does the Mute Nasal Dilator Help with Sleep? | Unboxing the Mute
Preventing the pooch belly
Question: Tips on preventing an alien from popping out when breathing after the brace.
Answer: Ahh, the classic pooch belly during the exhale. It’s something we especially see when we can’t get a complete exhale and closer at the lower ribcage.
When this deficit is present, there is a muscle that will try it’s darndest to compress the abdominal wall.
You guessed it…RECTUS (damn near killed us) ABDOMINIS.
When this puppy kicks in, it pulls the sternum downward, which creates an increase in downward pressure into the abdominal wall.
Don’t call Elenor Ripley fam, it’s not an alien. That pooch you are seeing is your abdominal contents being pushed anterior and inferior into the ab wall.
The solution would be to derectusify your exhale.
I talked about this on a previous post, but the three keys to getting a full exhale with minimal 6-pack action is:
1. Full, slow exhale that makes the ab wall smaller
2. Drive upper cervical extension
3. Choose positions where that doesn’t happen
If you want the full Monty, watch this video below
Quick tips on making nasal breathing easier
Question: How do I help my clients who feel like that can’t breathe well through their nose?
Answer: If your supreme clientele can’t breathe adequately through their nose, they might be onto something.
One could have difficulty eliciting the position and dynamics needed to achieve a full exhale, so you may have to help them out.
If you’ve coached the palatal tongue posture as we discussed above and nasal breathing is still a struggle, you can try a few simple things to make them nasal breathe like a BOSS!
1. Spread the nose
A quick and easy way to make nasal breathing hella easier is to have the client spread the skin on either side of the nose laterally. This helps increase the space available to breathe nasally.
2. Use nasal breathing appliances
You can also use various appliances to open up the nasal passages.
The cheapest entry point is the Breathe Right strip, which is basically an adhesive version of the nasal spread above.
If you want to kick it up a notch, a magnetized version of this product, called Intake Breathing, can be quite good also.
My personal favorite that I’ve used is the Mute, which is a nasal dilator that goes up your nose, opening the nasal passages. It’s great to exercise with. (I reviewed the Mute here.)
3. Saline rinses
Ya gotta keep them nasal passages clean, fam. Using nasal saline rinses can help open up the nasal passages. I would do this a couple of times per day.
4. Go see an ENT
If you’ve tried all of the above, and the effects are only temporary, you may need a more aggressive intervention. This would be where I would look into meeting up with an ENT who is breathing/sleep focused. Treatments could range from medication, surgery, allergy treatments, and other stuff I’m likely unaware of.
My ENT that I use is Dr. Soroush Zaghi.
Sum up
- Wide ISA – diaphragms are concentric anterior, eccentric posterior
- Narrow ISA – diaphragms are eccentric anterior, concentric posterior
- Getting the buckethandle action to occur requires keeping ab tension and ensuring the inhale is chill and relaxed
- Encourage nasal breathing throughout the day instead of the breathing excursions taught with stacking.
- Eliminate the pooch belly by exhaling slowly, making the ab wall smaller, extending the upper cervical spine, and choosing appropriate exercises
- Use nasal spreading, appliances, and washes to keep nasal passages open.