Table of Contents
Losing internal rotation may not be a shoulder problem
If you’ve been told you have GIRD, a forward head posture, or you slouch with reckless abandon, read on!
These issues are often linked to reduced shoulder internal rotation; a motion necessary for throwing, pressing overhead and reaching behind your back.
So the fix is to sleeper stretch and then the angels will sing right?!?!?!?

Uhh….no fam!
Instead, your whack shoulder motion can be profoundly influenced by altering dynamics within the ribcage.
The ribcage forms the base for your shoulder girdle. If you can’t move the foundation the way you want to, then you won’t be moving your shoulders the way you want to.
Ready to figure out assessing AND improving this important motion you and your clients NEED?
Then check out Movement Debrief Episode 134 below.
Watch the video below for your viewing pleasure, or listen to the podcast if you can’t stand the sight of me 🙁
and the audio version:
If you want to watch these live, add me on Instagram.

 t
tShow notes
Check out Human Matrix promo video below:
Below are some testimonials for the class:
Want to sign up? Click on the following locations below:
February 20th-21st, 2021, Atlanta, GA (Early bird ends January 17th at 11:55 pm!)
April 10th-11th, 2021, Warren, OH (Early bird ends March 14th at 11:55 pm)
May 29th-30th, 2021 Boston, MA (Early bird ends April 25th at 11:55pm!)
August 14th-15th, 2021, Ann Arbor, MI (Early bird ends July 18th at 11:55pm!)
September 25th-26th, 2021, Wyckoff, NJ (Early bird ends August 22nd at 11:55pm)
Dickinson College in Carlisle PA (POSTPONED DUE TO COVID-19) [Approved for 14 Category A CEUs for athletic trainers]
Montreal, Canada (POSTPONED DUE TO COVID-19) [6 CEUs approved for Athletic Therapists by CATA!]
Charlotte, NC (POSTPONED DUE TO COVID-19)
Or check out this little teaser for Human Matrix home study. Best part is if you attend the live course you’ll get this bad boy for free! (Release date not known yet 🙁
Here is a signup for my newsletter to get nearly 5 hours and 50 pages of content, access to my free breathing and body mechanics course, a free acute:chronic workload calculator, basketball conditioning program, podcasts, and weekend learning goodies:
[yikes-mailchimp form=”1″ submit=”Get learning goodies and more”]
ISA overview – Learn all things infrasternal angle with this post
Primary and Secondary Compensation – This post dives into which compensations you should focus on first.
Introduction to Myofunctional Therapy course review -You will learn all things upper airway when you dive into this post.
Airway Orthodontics with Dr. Hockel – Want to learn how a dentist can improve your sleep, forward head posture, and more? Then this post is a must-read.
Scapulohumeral rhythm – Learn how the scapula and humerus move during each phase of shoulder flexion.
Manubrial expansion – Here we discuss the best ways to improve mobility in the uppermost segments of the anterior chest wall.
Rounded shoulders and shoulder internal rotation
Question: How do I improve my shoulder internal rotation, and by that I mean dealing with shoulders that have rolled forward and not budging no matter what drill I try?
Answer: For visual reference, we are going to assume in this case the person in question has a depressed anterior chest, increased hinge in the thoracic spine leading to the appearance (not necessarily actual) of increased kyphosis, and a forward head position. See the picture below for reference:
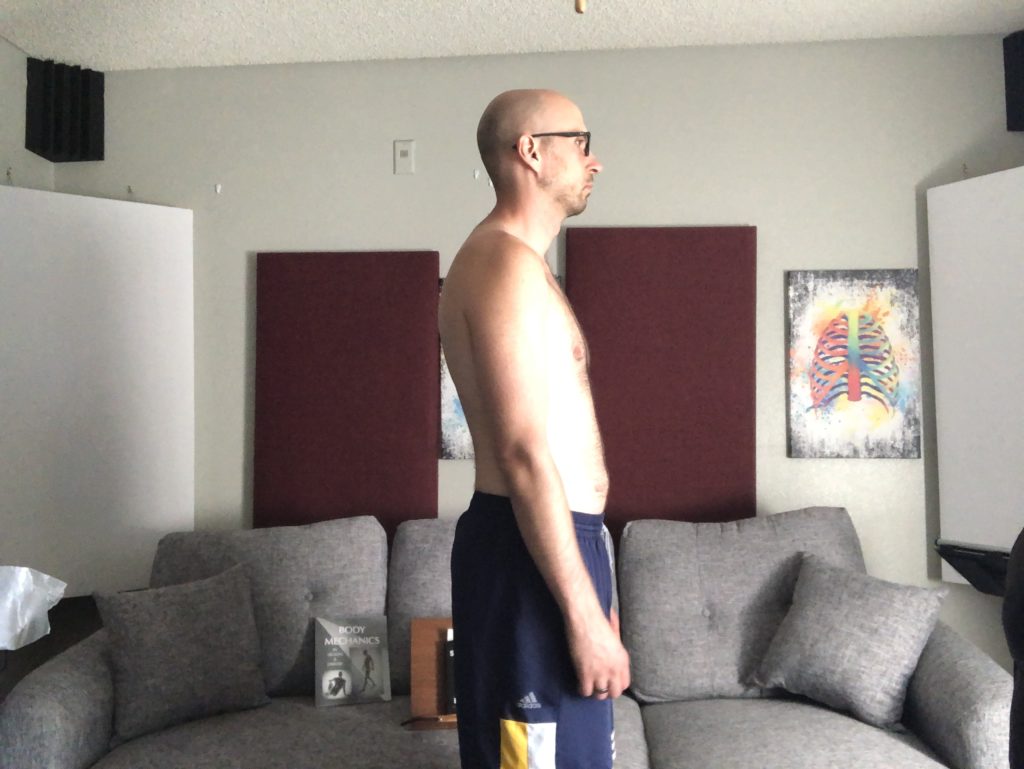
While there are several variations to this position (which will influence testing) and “causes,” the axial skeleton change that puts someone into this orientation is a concentric anterior thorax. This would be synonymous with a down pump handle or an inhaled axial orientation.
The sequence of the anterior thorax becoming concentrically oriented has an end result in decreased shoulder internal rotation. Here’s how the sequence happens:
- Concentric anterior thorax pulls shoulder blades forward (scapular abduction and internal rotation)
- Humerus externally rotates to position arm back to center (concentric external rotation).
- Humeral external rotation bias causes decreased humeral internal rotation
Before we go into what to do about it, it’s SUPER TOUGH and likely unnecessary to sweat changing static posture for a few different reasons:
- Postural presentations have structural influence. You can only change how you look insofar as your structure allows.
- We aren’t static creatures, we move. It is more important to be able to change into several different postures
- Sustaining any singular position for too long is undesirable. Lack of motion leads to tissue ischemia and problems
With that in mind, let’s first look at what we need to do to improve the dynamics of this presentation.
Thorax treatment for rounded shoulders
The first line of defense should be to improve thorax movement options and shape. If the pump handle is down, we need to raise it up like Josh Groban!
To improve movement in this region, the best choice is to do one of the following:
- Reach between 60-120° of shoulder flexion
- Drive shoulder extension and scapular retraction
Exercise choice will depend on which infrasternal angle presentation (ISA) you are dealing with, as this changes the “cause” of this position.
- Narrow ISA: concentric anterior thorax is due to skeletal structure (primary compensation)
- Wide ISA: concentric anterior thorax is a secondary compensation.
Therefore, what you go after changes with each presentation. For the narrow ISA, you need to restore structural dynamics to elicit a change. A narrow ISA has reduced lateral ribcage dimensions, so you need to do things to expand that. A forward reach can be useful in this regard:
If we did the above move to a wide ISA, who has increased lateral ribcage dimensions, this would not be the best choice to improve ribcage dynamics. If you reach between 110-120° of shoulder flexion, the serratus anterior will aid in lateral ribcage compression:
Once you’ve got these moves on point, and need to clean up the last bit, driving shoulder extension with scapular adduction can drive more air in the front:
Cervicocranial treatment for rounded shoulders
Now I would be remiss to say there aren’t upper airway influences to this bias. Rounded shoulders are often associated with a forward head posture. A forward head posture can be a compensatory action for the inability to nasal breathe:
- You can’t breathe through your nose for whatever reason
- Tongue posture sits low to open the oral airway
- Forward head posture occurs to increase airway size
- Depressed hyoid position occurs
Now, diving into ALL the possible treatments goes beyond this post, but myofunctional therapy can play a major role in improving dynamics in this region.
The two major keys you will need to focus on will be:
- Attaining a palatal tongue posture
- Elevating the hyoid
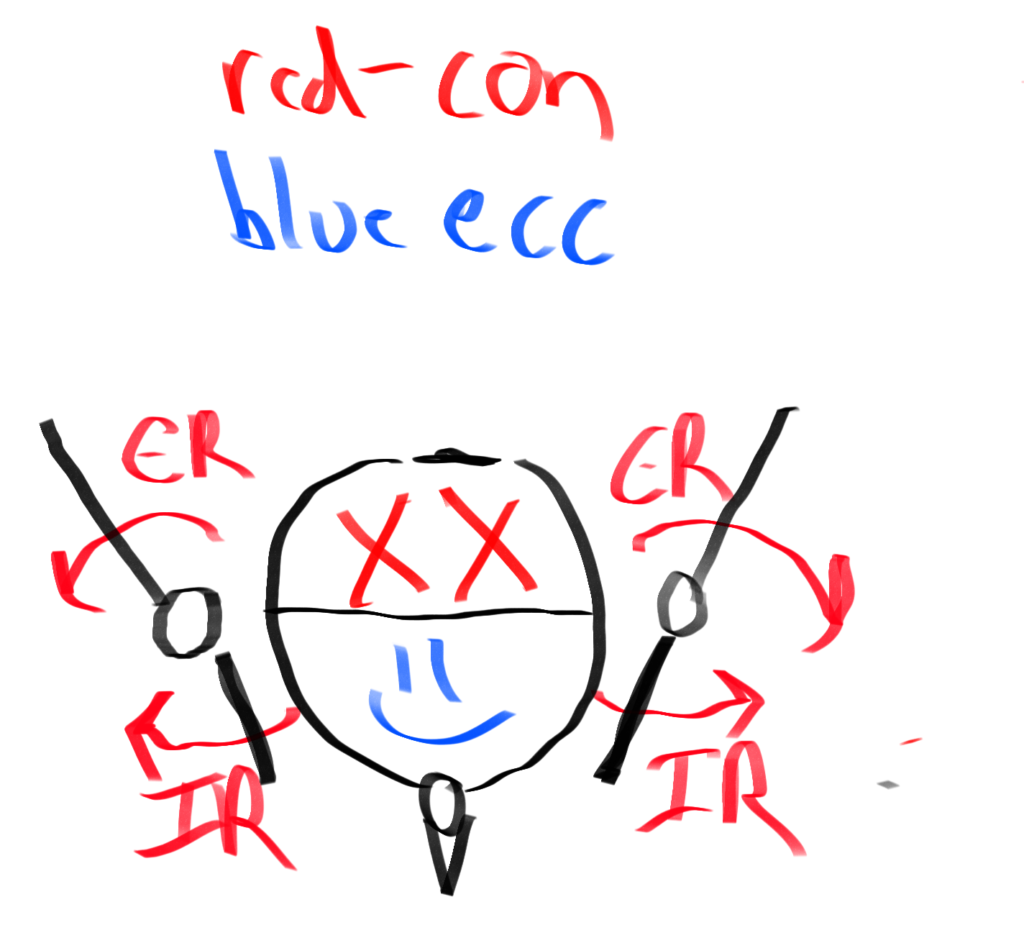
For palatal tongue posture, this involves placing the tongue on the roof of the mouth and holding it there. Simply working on clucks can improve this position:
If you want to get ya hyoid up, son, then you need to get your swallow on point! The smiling swallow is an excellent drill to focus on this limitation:
Exercises for shoulder internal rotation
Question: If someone is missing shoulder IR, how do you decide if you load an exercise either in the suitcase/low hold position or the goblet position
Answer: As we mentioned above, shoulder internal rotation restrictions are likely due to a concentric anterior thorax. The treatments (uh, hopefully, you know from above fam!) would be to place your arms in one of the following positions:
- Reach between 60°-120° of shoulder flexion
- Drive shoulder extension and scapular retraction
The goblet position is roughly between 70°-90° of shoulder flexion, so I think it’s pretty easy to see how that can help improve internal rotation, but what about the suitcase position? How do those lovely suitcase carries influence thorax dynamics?
I’m glad you asked!
The reason why suitcase carries are useful activities has little to do with the weight side. The #majorkey is actually the swing arm.
When you swing your arm to and fro, you are driving trunk rotation. Since the weighted arm is minimally moving, it gives your trunk a fixed point to rotate about; making the suitcase carry money for anteroposterior expansion.
Where air will go depends on what arm swing position you are dealing with:
- Arm forward rotates trunk contralaterally
- Arm backward rotates trunk ipsilaterally
The trunk rotation direction will influence where the air will go:
- Left rotation: Expansion left posterior and right anterior thorax
- Right rotation: Expansion right posterior and left anterior thorax
Since you’ll rotate both directions with the suitcase carry, you’ll get a bit of air EVERYWHERE. That’s why I coach the suitcase carry as such:
If someone has difficulty keeping the stacked position on the suitcase carry, working drills that drive hip extension and humeral extension can prove useful, as these actions will challenge your ability to keep the stack in this move. Split squat variations come to mind:
Pec minor strain
Question: Can u do something on pec minor strain (right side). Seems to keep recurring every time I perform any chest exercises. Keep up the good work!
Answer: First, let’s look at the pec minor anatomy.
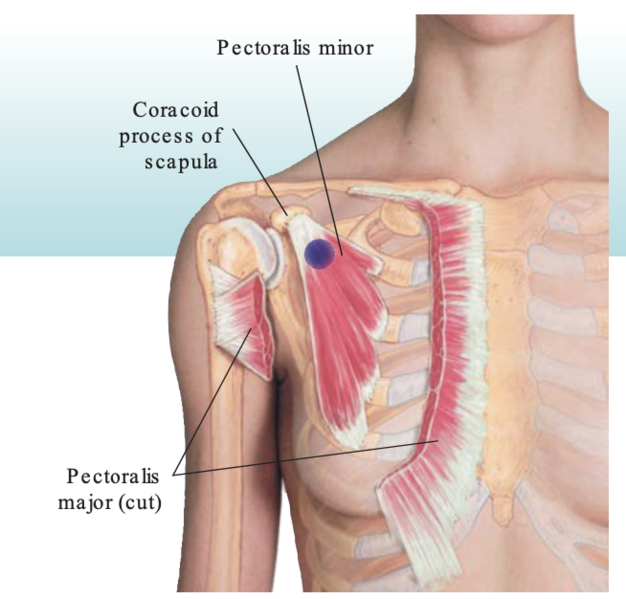
- Proximal attachment: ribs 3-5
- Distal attachment: coracoid process of the scapula
- Actions: elevate ribs (pump handle), downwardly rotate and protract the scapula
Now if you doing HELLA chest work because you want them pecs like whoa, then that may contribute to the concentric bias of the anterior chest wall. This bias would make pec minor eccentric proximally. Couple that with pulling the shoulders back for bench press and such, and you get a stretched AF pec minor. This could be a contributing factor to the strain.
The solution is simple: get air into the chest to drive some concentric activity into the pec minor. Hell, even get some reaching forward to protract the scapula. Put the pec minor in the orientation it’s not in. This will restore contractile options in the pec.
A great move would be any type of forward reach:
Horizontal adduction
Question: You mentioned limitations in horizontal adduction. How do you assess this? Are you just holding the ribcage down and then adducting the arm until the ribcage starts coming up? Or are you holding the scapula down?
Answer: You want to isolate the movement to the humerus. The big issue that will happen when you run out of humeral room is the scapula will go along for the ride.
And I don’t want the scap in my car 😉
So, you’ll want to pin the scapula down with your thumb. Then pull the humerus across the body. You are looking to get the olecranon to get slightly past the nose, which is about 135°.
Horizontal adduction measures T2-4 anterior expansion, so you’ll want to drive stuff that involves the following:
- Horizontal adduction
- Humeral extension
- trunk rotation
One of my favorites that has been killing it because of the cervical rotation component has been the sidelying armbar. I’ll even do this as an iso, it’s been that good:
Abdominal overactivity during exhales
Question: What do you do about ab overactivity on exhales?
Answer: Generally, if you see too much abs during the breathing sequence, there are a few simple tricks you can do to get the abs to chill.
- Make sure the tuck is ab-less.
A lot of times, peeps will kick in the abs to perform the tuck instead of the glutes and hamstrings. This will then lead to further concentric activity of the abdominals during the exhale.
WE DON’T WANT THAT!
So ensuring that they can get a tuck without kicking in the abs is WAY important. Working on a hooklying tilt progression can be a great way to teach this action:
2. Exhale slower
Most people exhale WAY too quickly, which will greater bias superficial abdominal musculature, limiting your desired thorax expansion.
I usually tell these people to either go 50% slower than what they did, or make the exhale be 15 seconds long. No one will exhale for 15 seconds, but they’ll get the idea.
3. Use prone or quadruped
When your stomach is facing the ground, gravity will push the viscera anteriorly into the ab wall, thus creating an eccentric abdominal orientation.
Sum up
- Rounded shoulders are caused by a concentric anterior thorax, which reduces humeral internal rotation.
- Reaching 60°-120°, humeral extension, trunk rotation, and horizontal adduction can all improve anterior thorax mobility.
- Reduce pec minor strain by driving air into the anterior thorax and reaching.
- Horizontal adduction is tested by pinning the scapula down and going across the body.
- Reduce ab overactivity by tucking without abs, exhaling slower, and using prone/quadruped.