Table of Contents
If there is a frontal plane problem, you will want to check this out
Are you someone who has a lateral pelvic tilt, a lateral spine shift, or Trendelenburg gait.
If so, then this is the post for you, because we outline what is going on movement-wise, and what the heck you can do about it.
Check out Movement Debrief Episode 156 below to learn more.
Watch the video below for your viewing pleasure.
Or listen to my sultry voice on the podcast version:
If you want to watch these live, add me on Instagram.
Show notes
Check out Human Matrix promo video below:
Below are some testimonials for the class:
Want to sign up? Click on the following locations below:
September 25th-26th, 2021, Wyckoff, NJ (Early bird ends August 22nd at 11:55 pm)
October 23rd-24th, Philadelphia, PA (Early bird ends September 26th at 11:55pm)
November 6th-7th, 2021, Charlotte, NC (Early bird ends October 3rd at 11:55 pm)
November 20th-21st, 2021 – Colorado Springs, CO (Early bird ends October 22nd at 11:55 pm)
December 4th-5th, 2021 – Las Vegas, NV (Early bird ends November 5th at 11:55 pm)
Or check out this little teaser for Human Matrix home study. Best part is if you attend the live course you’ll get this bad boy for free! (Release date not known yet ?
Here is a signup for my newsletter to get nearly 5 hours and 50 pages of content, access to my free breathing and body mechanics course, a free acute:chronic workload calculator, basketball conditioning program, podcasts, and weekend learning goodies:
Full Name Email AddressGet learning goodies and moreEdit Form | Customize Form
Fixing lateral pelvic tilt
Question: Can you do some videos on how to correct a lateral pelvic tilt with breathing techniques?
Answer: A lateral pelvic tilt is where one side of the pelvis appears higher than the other. Sometimes this can be structural because of differences side-to-side in pelvic morphology, other times it can manifest because of reductions of movement.
Since we can’t change how you look inside, and we can’t accurately measure it, we are going to look at the movement side of the equation.
First things first, the ability to tilt the pelvis laterally is normal. As in fam, this is a normal movement that we have the capability of performing. If you have ever seen that Reno 911 drunk driving skit, you’ll know what I’m talking about.
In order for this lateral tilt to occur, we need the following actions to be able to happen in the lower body:
- Sacrum nutates with a slight turn towards the tilted side
- Pelvic outlet abducts
- Femur adducts and internally rotates
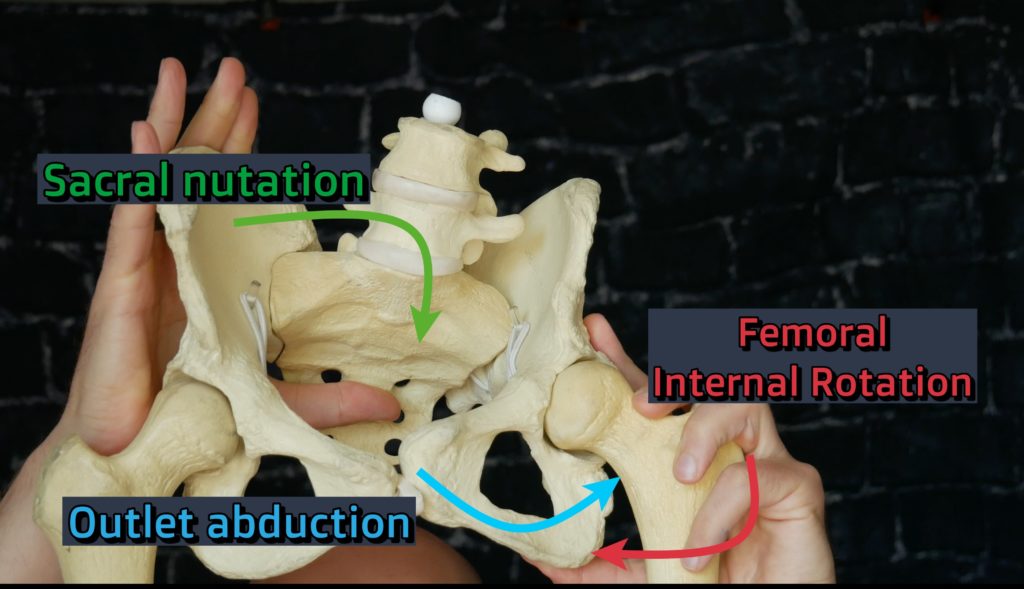
All of the aforementioned actions create an internal rotation action through the lower extremity, and it’s commonly seen in the midstance of gait.
If you can’t do these actions for whatever reason, your body may have to utilize some type of compensatory strategy to make that happen.
Think of it this way, the body is going to try and change it’s orientation to where there is available space to move and demonstrate this action. There are many ways this can be done.
The most common way to “make up” for an internal rotation deficit is by tilting the pelvis anteriorly, as this will change the pelvic orientation so more internal rotation can be acquired.
If you notice a lateral pelvic tilt on either side, then you are likely dealing with varying degree of anterior pelvic tilt on one side of the other.
Now fam, we have to appreciate that these tilts could occur differently on either side. Because of our internal organ asymmetry and the normalcy of having a right-sided bias within our spines, the lateral tilt likely will not occur in the same way from left to right.
Let’s first start with the left side, since it’s the WAY COOLER side (trust me, I’m left-handed).
The left is also easier to see and think about, as it “fits” the rightward turn that our spine has. In order for this tilt to appear the pelvis on the left will move forward and obliquely to the right (this is called a right oblique pelvic orientation according to Daddy-O Pops Bill Hartman). The pelvis orients in this fashion on this side to not push an internal rotation range that can be achieved. You’ll know if you have this orientation if your straight leg raise on the left is greater than the right.
When the right pelvis is tilted higher than the left, the pelvic turn is actually still to the right, only it is flatter and not on an oblique axis.
In this case, both sides of the pelvis will be moving forward at a more equal rate, but the flatter turn allows the right side of the body to have more of an internal-rotation bias in comparison to the left both in the pelvis and the thorax. The combination of the right pelvic outlet abducting and the thorax right side bending gives the appearance of a right lateral pelvic tilt. Your telltale sign will be the right straight leg raise being greater than the left.
Cool fam, so we know what the heck is going on, what is a fam to do about it?
I’m…glad….you….asked.
Regardless of either case, stacking the thorax atop the pelvis is a rock-solid starting point. Since both presentations have an anterior tilt about them, you gotta pull that bad boy back to allow for any rotation to occur.
I would practice all of the moves from my stacking starter pack to get the ball rolling here.
Once you’ve done that, let’s now look at how to improve movement in each of these cases.
Treating a left lateral pelvic tilt
Remember, a left lateral tilt occurs because of the pelvis rotating obliquely to the right, so we have to reverse engineer this position.
Our first step is to get the pelvis to turn to the left. We can use the right side of our body to push back to the left. Given that the left posterior lower pelvis is eccentric (that cray cray straight leg raise, remember), and also given that you generally want to restore external rotation measures before internal, you’ll want to perform an action on the right side to get yourself some external rotation back.
A great move here is a sidelying stride:
Once you’ve nailed that, you then want to teach your supreme clientele to posteriorly tilt the left side and turn the sacrum to the left. At higher degrees of hip flexion, this will help “close” the lower posterior outlet. A posterior hip stretch on the left would do wonders here:
Treating a right lateral pelvic tilt
Don’t forget big fam, a right lateral tilt is more of a flat pelvic turn. There is more space available on the right posterior side, so treatment here is essentially going to be closing the right posterior and opening up the left anterior.
You can achieve this with something where it’s more of a shift in the 90 degree range. A sidelying hip shift on the left can be great here:
Gym-wise, you could similarly drive this position with either a shifted RDL:
And eventually progress to a split squat with contralateral hold:
Lateral shift
Question: Can you make a video about lateral shift?
Answer: Why yes, yes I can 🙂
First, we have to understand what exactly is going on with a lateral shift. Essentially, a lateral shift is a short-term scoliosis strategy that manifests as a way to offload any affected structures. It is commonly associated with disc injury, but not always, and can occur either side of injury.
Before proceeding with any treatment on this, you have to make sure you get checked out by a medical professional to rule out any serious pathology. If you are getting any pain, weakness, sensation loss, etc down the leg, well fam check that out first! Sometimes doing something quick to reduce inflammation medically can make a world of difference.
But let’s say you got checked, aggressive treatments are not indicated, what the heck do you do for this lateral shift.
We have to look at when I shift laterally, what range of motion is often lost in this case.
It’s not uncommon for a straight leg raise to be limited in this population. Moreover, sidebending maneuvers, at least based on what these occur in gait, are associated with more of an internal rotation-based strategy in my opinion.
Therefore, if I sidebend in one direction, I will pick up internal rotation towards the sidebend, and reduce it away from the sidebend. If I have less internal rotation, there will be less compression over the given area.
What I’ve found useful in these cases is to choose activities where you are doing your darndest to create some type of internal rotation restoration.
The two big keys would be to perform some type of shift towards the affected side, like a sidelying hip shift:
Then doing something to create lateral expansion of the ribcage. Something like this swiss ball stretch can be useful:
Trendelenberg gait
Question: How would you tackle trendelenberg gait?
Answer: Trendelenberg gait is where there is some issue with the hip abductors that causes a drooping of the hip towards the stance side. This issue commonly happens when there is neurological weakness from back issues or after hip surgeries that didn’t go so well.
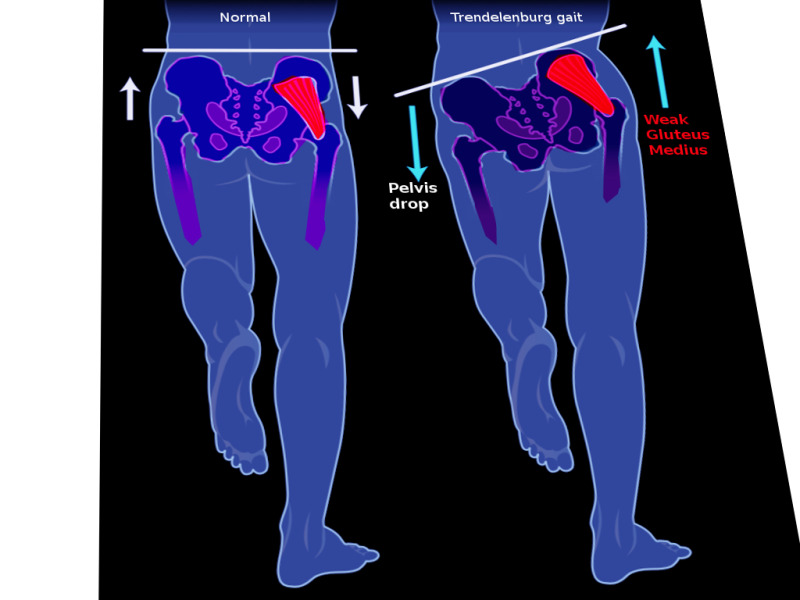
Assuming you’ve ruled out structural issues, we have to look at what phase of gait this issues happens, and generally that’s midstance.
During midstance, the pelvic outlet needs to abduct, which helps create more ipsilateral adduction and internal rotation of the femur.
If the above action can’t happen, the pelvis orients in a way that drives a CRAZY amount of adduction and internal rotation. That, my dear fam, is your trendelenberg sign.
So, what we are to do is to get the outlet to open when we need to big fam. Anything that teaches this action to occur is useful. Your classic hip hike exercises actually work pretty slick here:
Sum up
- Lateral pelvic tilts and shifts occur to orient the body so internal rotation can be expressed
- Actions to increase internal rotation, which include stacking, frontal plane shifting, and rotational shifts, can be useful to increase these positions.