
Table of Contents
Let’s navigate through compensations seen not just the ankle, but up the chain!
Do you have ankle problems? Done a bunch of wall ankle stretches to no avail?
Perhaps you have to look elsewhere. Namely, how ankle restrictions link up through the rest of the body. How are ankle limitations commonly seen manifested through common compensatory strategies?
That’s what we dive into in today’s post. Check out Movement Debrief Episode 155 below to learn more.
Watch the video below for your viewing pleasure.
Or listen to my sultry voice on the podcast version:
If you want to watch these live, add me on Instagram.
Show notes
Check out Human Matrix promo video below:
Below are some testimonials for the class:
Want to sign up? Click on the following locations below:
September 25th-26th, 2021, Wyckoff, NJ (Early bird ends August 22nd at 11:55 pm)
October 23rd-24th, Philadelphia, PA (Early bird ends September 26th at 11:55pm)
November 6th-7th, 2021, Charlotte, NC (Early bird ends October 3rd at 11:55 pm)
November 20th-21st, 2021 – Colorado Springs, CO (Early bird ends October 22nd at 11:55 pm)
December 4th-5th, 2021 – Las Vegas, NV (Early bird ends November 5th at 11:55 pm)
Or check out this little teaser for Human Matrix home study. Best part is if you attend the live course you’ll get this bad boy for free! (Release date not known yet ?
Here is a signup for my newsletter to get nearly 5 hours and 50 pages of content, access to my free breathing and body mechanics course, a free acute:chronic workload calculator, basketball conditioning program, podcasts, and weekend learning goodies:
Full Name Email AddressGet learning goodies and moreEdit Form | Customize Form
Turned-in ankles with knee valgus
Question: I have a client who has turned in ankles. This affects her hips as her knees cave in. She has strength in her quads but can not perform the hinge movement or squats properly. I’m not sure how I can help her?
Answer: What we are seeing here fam is a twist, and not the cool Chubby Checker kind.
I’m talking about a twist of the distal femur going in one direction, and the tibia in another.
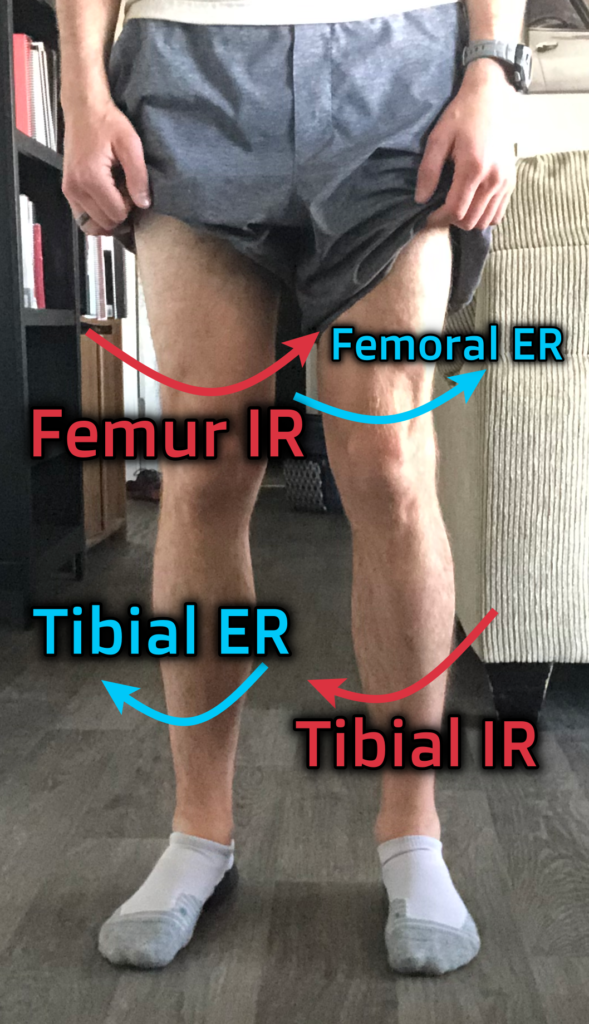
If the knee is caving in and the ankle is inverting, you have a situation where the distal femur is internally rotating, and the tibia is externally rotating:
When you see a twist like this, it is not uncommon for knee flexion to be limited, as this position is also the screw home position that occurs with knee extension. Which fam, you kinda sorta need to bend your knee when you squat and hinge.
I talk about how to untwist legs in this post, but we basically have to look at reversing this mechanism. But in order to teach this person’s body to go the other way, we have to start up top. The pelvis
If you are seeing knees caving in like cray, there is a good chance the pelvis is anteriorly tilting/orienting. This position allows more internal rotation to occur, but at the consequence of losing available relative motion between joints.
So first, you must reorient the pelvis. Teach some posterior tilting aka the tuck. This hooklying tilt progression is a great starting point for most:
I would also get WAY good at my stuff on the stacking starter pack:
Once your client is a bad mother tucker. You can then start working on “untwisting” the knee joint and altering ankle position. To untwist, you have to drive the following movements:
- Femoral external rotation
- Tibial internal rotation
- Foot/ankle pronation
These movements naturally occur at either small amounts of knee/hip flexion or all the way at end-range knee/hip extension. Since this client struggles with squats and hinges, it probably makes sense to start with something higher depth. A squat variation with a band around the knees (only light pressure) while keeping inside heel contact could be money:
Once you got this, we can then push into the troubled range. Mid-depth squats and deadlifts require internal rotation, so we want to try and maintain leg position when we go here. Doing a split squat while keeping the knee out and inside foot contact is a great place to go:
To really crush things depth wise, you can progress to all the way at the bottom position of a split squat. We are talking internal rotation city fam! I would start with this half kneeling progression, really emphasizing the twist:
Your terminal move should be the bottoms up shifty split squats. This move is an absolute monster, but you can bet that your squat is going to reach BOSS status:
Now fam, I’d be remiss to say it would probably be worthwhile to continue training the squat as you work through this progression. By elevating the heels on a ramp, you bias the entire leg to external rotation, which will make your life WAY easier when it comes to squatting.
You can start with a ramp goblet squat
Then progress to something like a zercher:
You do that, and NO ONE will mess with you J
The link between ankle dorsiflexion and hip internal rotation
Question: I’m having problems with ankle dorsiflexion on my right side. It feels blocked at the talus and I often even hear and feel clicking in that area. I Also notice that the medial maleolous is more prominent on that side almost like there is excessive tibial internal rotation?
I was doing movement screening and realized my hip internal rotation on that same side was very restricted, so I started working on that and noticed that it helped both of those symptoms in my ankle!
I still have a lot of stiffness on dorsiflexion though and though I’ve been working in the hip for about 2 weeks now I seem to still be stiff every morning until I do my 90/90 hip lift and work on the hip IR.
Is there anything you recommend doing for this situation and how long till I see lasting changes or maybe how should I program working on this issue? Thanks!
Answer: JD here found a dope link between ankle and hip motions. Namely, as the ankle dorsiflexes and everts, the hip must internally rotate. You can see this link by simply everting and dorsiflexing and watching where your knee goes.
JD is also correct in that medial malleoli prominence corresponds with tibial internal rotation. This orientation is likely the way that he gets internal rotation to occur throughout his extremity when he needs it, especially if we aren’t seeing a whole lot at the ankle and the hip. With this presentation, there could be a few different possibilities:
- There could be bone growth at the medial malleoli, which we can’t change (Wolff’s law fam!)
- The foot could be “stuck” in a supinated position (external rotation), limiting dorsiflexion, with the internal rotation occurring solely at the distal tibiofibular joint
- The subtalar joint could be limited in eversion (external rotation orientation) and the midfoot and distal tibiofibular joint could be pronated (internal rotation)
In any of these cases, the intervention remains the same:
Teach this leg internal rotation.
You could totally use the previous progression we discussed in the last question, making sure to really emphasize calcaneal eversion and foot pronation. I’m talking TONS of inside heel and arch contact.
The only tweak I would make to the above progression is potentially using ramps for every move. This addition would limit the dorsiflexion demands, especially if big fam over here has very little dorsiflexion.
Muscle strengthening after ankle surgery?
Question: Do you do any kind of muscle strengthening for someone coming off a lateral ligament reconstruction. A lot of times I have pain trying to dorsiflex with my weight but not if I support my weight.
Answer: When I approach post-operative care, the only things that differ in the process are the following:
- Respek (not a typo, fam) tissue healing times and subsequent precautions.
- Control for the inflammatory process by all means necessary.
After that, the song remains the same. You are still trying to restore movement options locally and systemically with whatever modalities work. This could include manual therapy, exercise, whatever.
The first line of defense should be driving any movement restrictions that are present. If motion is limited, your strength work will also be limited. If you need to drive the paired mechanics of plantarflexion and inversion, this move is great during the nonweightbearing phase:
VID – adduction
High depth hip shifts are great once you are weight-bearing:
For dorsiflexion and eversion with nonweight-bearing, sidelying hip abduction with calcaneal eversion is rocking:
If you need dorsiflexion and eversion in the weight-bearing phase, look no further to the progressions from the previous question
Now if you can do all these moves without any issues, your ankle will probably be strong as all hell. A solid loaded squat probably won’t be aided much by band resisted eversion.
Now if by some chance you do all this stuff and there is a local strength issue at the ankle, then perhaps band work is useful. I could also see this being possible if hypertrophy in the nonweight-bearing phase is the goal. Combine this with blood flow restriction training, and you might be onto something.
That said, the need for local strengthening other than the aforementioned cases is to me is quite rare. The one exception would be neurological conditions, such as weakness after a back injury. Even here, I would be considering blood flow restriction and possibly manual PNF work to return some force production.
It could be, in JD’s case, that it’s harder for him to drive the internal rotation mechanics needed during dorsiflexion. Supporting his body may just make this position easier.
Haglund’s deformity
Question: How to fix an ongoing issue with a bone growth on my heel affecting the insertional point of my achilles, resulting in continual soreness when running, please.
Answer: The bone growth our fam is reference is called a “Haglunds Deformity,” which is basically a large process on the upper part of the calcaneus. Theoretically, this deformity may impinge on the calcanea bursa, which could cause pain at the achilles tendon insertion (study I’m pulling from here).
Now the first question we have to ask is does this growth actually cause insertional achilles tendinopathy, that is, pain at the tendon’s distal attachment?
Well, according to the same study from above, this deformity was equally present in asymptomatic patients and similar in structure. Now it’s only one study, but that leads me to thinking we cannot say to what extent the Haglund deformity affects symptoms, if at all.
Moreover, you cannot change bony structural adaptations, so why sweat it unless surgery will be performed. But according to this paper, the results are not spectaular. Complete relief occurred in less than 70% of subjects, with a 6 month to 2 year recovery time.
So if surgery is out, what the heck can we do about insertional achilles tendinopathy??
I’m glad you asked!!!!!
The treatments would be very similar to concepts discussed in all the above cases. Restore movement options in the lower extremity to may reduce any torsional strains on the tendon. This caller also mentioned discomfort with running, so it may be wise to reduce mileage or even rest until this calms down. Load management is immensely critical for any type of tendon issue, so making sure symptoms calm down is important.
Lastly, utilizing isometrics for symptom relief can be quite useful. You may consider isometric plantarflexion in a heavy loaded calf raise machine as a money move to reduce symptoms. With insertional achilles tendinopathy, you would not push as much into a dorsiflexed position. You’d want the heel raise to be to flat, as this will reduce the pull on the insertion and be more comfortable. From there, you’d progress loading to slow speed then fast speed in the same vein.
If you want to see a full progression, I would definitely check out this post.
Supination, pronation, and infrasternal angles
Question: Could you explain pronation and supination and which infrasternal angle presentation is associated with each?
Answer: Pronation is associated with internal rotation, and supination is associated with external rotation. You can see this relationship by driving either in your foot, and watch where you knee goes.
We then have to work our way up the chain to see what the pelvis is doing. Below are the following links:
- Supination –> external rotation –> sacral counternutation
- Pronation –> internal rotation –> sacral nutation
With the above sacral orientations, the narrow infrasternal angle has more of a counternutation bias, and the wide infrasternal angle has more of a nutational bias. And that, my fam, is how supination and pronation are linked to infrasternal angles. Narrows have more of a supination bias, and wides a pronated bias.
If you see the opposite of these orientations, then you are likely dealing with secondary compensations.
Sum up
- Knees caving and ankles flopping out require twisting the legs in opposing directions; work through split squat progressions to nail it!
- Limited ankle dorsiflexion requires driving calcaneal eversion, hip internal rotation, and ankle dorsiflexion simultaneously.
- Local ankle strengthening is rarely indicated unless it’s nonweightbearing phase or for neurological injuries. Restoring loaded global movement patterns often takes care of enough.
- Haglund’s deformities are not always associated with insterional achilles tendinopathy. The best bet is load management, restoring movement options, and progressing loading safely.
- Supination is often associated with narrow infrasternal angles; pronation with wide infrasternal angles.