Tag: straight leg raise
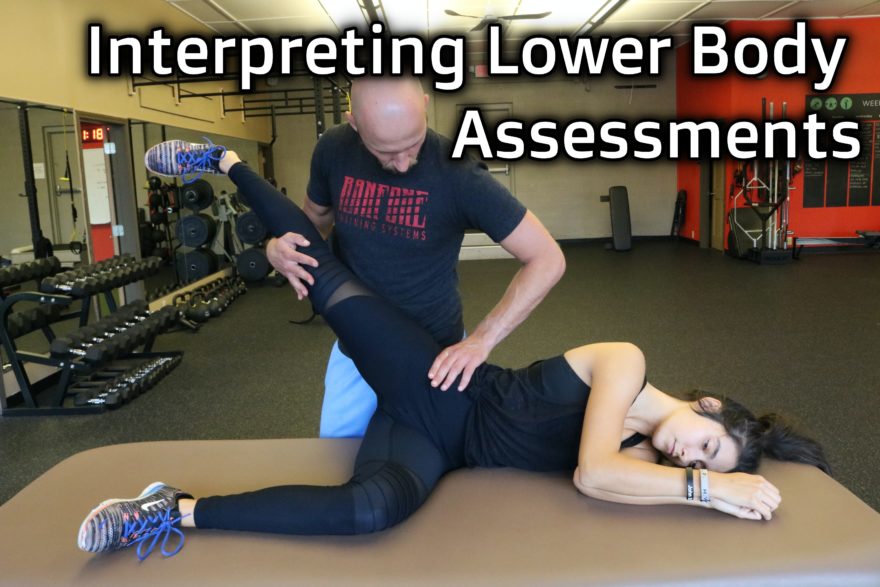
Interpreting Lower Body Assessments
How to go through common lower body assessments Movement Debrief Episode 114 is in the books. Below is a copy…

Challenges of Home Exercise Execution, Do You Really Have Sagittal Plane? and PT in 25 Years – Movement Debrief Episode 17
Just in case you missed last night’s Movement Debrief Episode 17, here is a copy of the video and audio…
Master Sagittal Plane, Coaching Progressions, Detaching, & TFL Inhibition – Movement Debrief Episode 5
Did you miss Movement Debrief live yesterday? Though much more fun live, I have a video of what we discussed…

90/90 Hip Lift – A Movement Deep Dive
The Fundamental Rehab Technique It’s a classic that does so much more than the naked eye can see. This round…

The Ultimate Guide to Treating Ankle Sprains
A Humdinger No Doubt Ankle sprains. Such a bugger to deal with. Ankle sprains are one of the most common…
The Sensitive Nervous System Chapter X: Neurodynamic Tests in the Clinic
This is a summary of Chapter X of “The Sensitive Nervous System” by David Butler. The Tests When assessing neurodynamics,…