Table of Contents
A deep dive into pelvic floor biomechanics
Breathing is super important you know, but the base of breathing is the pelvic floor.
Well fam, what if you don’t have the biomechanics on point down there?
Then you’ll need some help! We will sift through it in this post.
Check out Movement Debrief Episode 157 below to learn more.
Watch the video below for your viewing pleasure.
Or listen to my sultry voice on the podcast version:
If you want to watch these live, add me on Instagram.
Show notes
Check out Human Matrix promo video below:
Below are some testimonials for the class:
Want to sign up? Click on the following locations below:
September 25th-26th, 2021, Wyckoff, NJ (Early bird ends August 22nd at 11:55 pm)
October 23rd-24th, Philadelphia, PA (Early bird ends September 26th at 11:55pm)
November 6th-7th, 2021, Charlotte, NC (Early bird ends October 3rd at 11:55 pm)
November 20th-21st, 2021 – Colorado Springs, CO (Early bird ends October 22nd at 11:55 pm)
December 4th-5th, 2021 – Las Vegas, NV (Early bird ends November 5th at 11:55 pm)
Or check out this little teaser for Human Matrix home study. Best part is if you attend the live course you’ll get this bad boy for free! (Release date not known yet ?
Here is a signup for my newsletter to get nearly 5 hours and 50 pages of content, access to my free breathing and body mechanics course, a free acute:chronic workload calculator, basketball conditioning program, podcasts, and weekend learning goodies:
Full Name Email AddressGet learning goodies and moreEdit Form | Customize Form
Pelvic floor biomechanics
Question: Make a video on both sides of the pelvic floor spectrum, concentric orientation and eccentric.
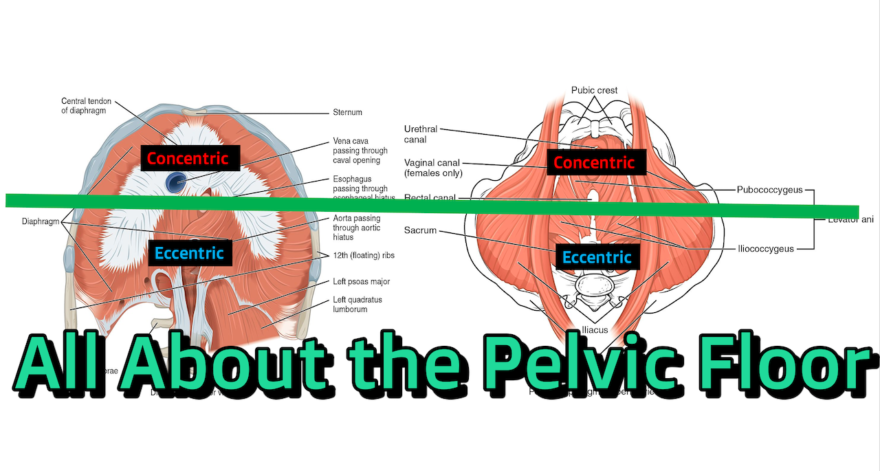
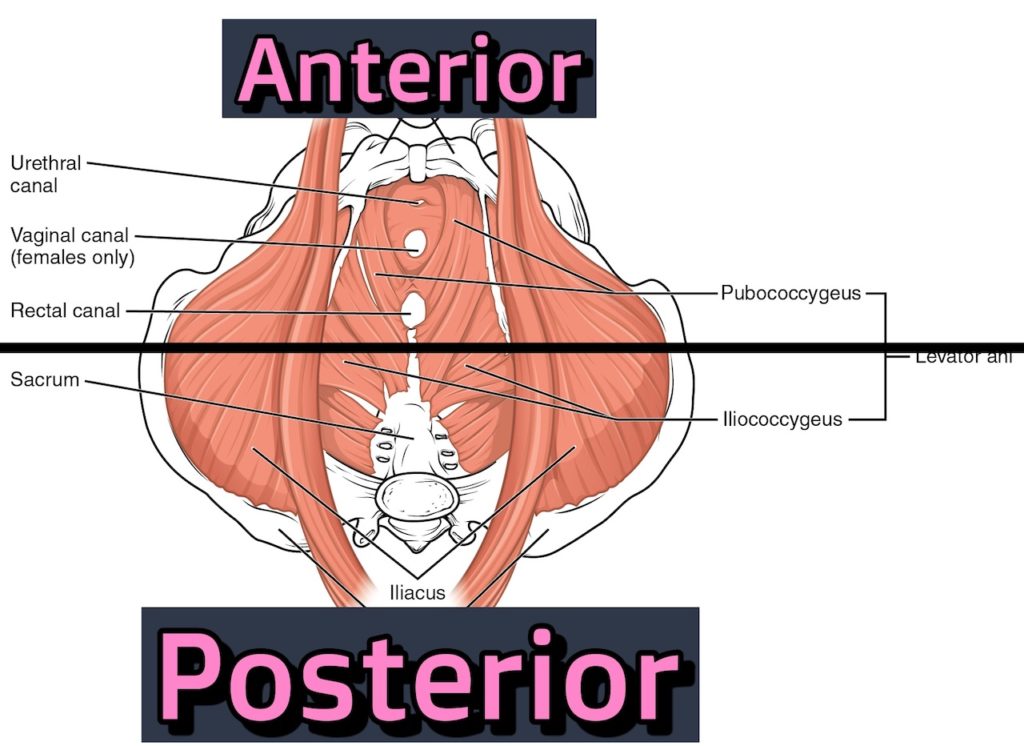
Answer: To keep it simple AF, we will break the pelvic floor into two sections: anterior and posterior.
{kind=link}
Looking at the pelvic floor in this fashion can assist us in determining how the pelvic floor behaves when sacral movements (and breathing) occur.
Although the movement of the sacrum isn’t a whole lot (like 2ish degrees), that doesn’t mean that the tissues don’t pull on the bones accordingly, fam!
With that in mind, there are two movements that occur at the sacrum: nutation and counternutation
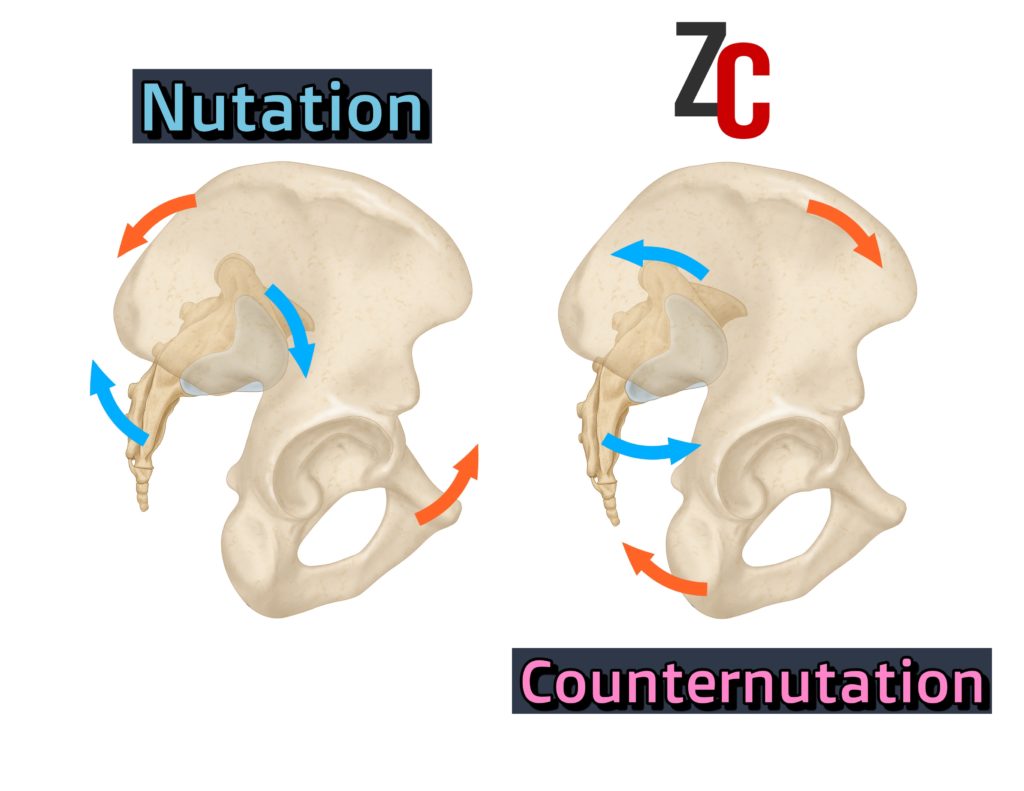
Sacral nutation involves the sacrum tipping forward and the innominates rotating posteriorly. Given the relative motions between the two bones, the pelvis orients more forward in this case.
Sacral counternutation reverses that action; sacrum tips backward and innominates rotate anteriorly.Given the relative motions between the two bones, the pelvis orients more backward in this case.
That’s the general sacral movements, now we have to ask ourselves how is the pelvic floor involved in these movements. To understand how this occurs, we have to look at these sacral actions from the bottom up. Through the outlet. In through the outlet, sounds like a nerdy Led Zeppelin album.
ANYWAYS!
When the sacrum nutates, the bottom of the sacrum, coccyx, will move posteriorly. In order for this bone to move posteriorly, an eccentric contraction of the posterior pelvic floor must occur. To create a gradient for the posterior pelvic floor to move to, the anterior pelvic floor concentrically contracts.
Therefore:
Sacral nutation = eccentric posterior pelvic floor + concentric anterior pelvic floor
As you can imagine (because who doesn’t imagine pelvic floor musculature!), the reverse will be true for counternutation. Here, the coccyx approaches more the middle. This position happens when the posterior pelvic floor creates a concentric contraction, and the anterior pelvic floor an eccentric contraction.
Ergo,
Sacral counternutation = concentric posterior pelvic floor + eccentric anterior pelvic floor
Now if you’ve been following ya boi for a hot minute, you might be thinking about how certain structural biases we have (aka how we are built aka anthropometrics aka infrasternal angle aka fam!) influence these sacral dynamics.
Well basically, certain peeps are going to have an easier time nutating, and others will counternutate like it’s nothing.
Who are those respective people?
I’M GLAD YOU ASKED!!!!!!!!
This, folks, is where we look at infrasternal angle presentations. The skeletal structure one has can potentially influence the sacral position one has, and subsequently the contractile bias of the pelvic floor.
These positions likely mirror what occurs in the thoracic diaphragm. In those with wide infrasternal angles (>90 degrees), the anterior thoracic diaphragm is concentric, and the posterior diaphragm is eccentric.
Given how the viscera downwardly displace in this situation, you’ll have a nutated sacral position associated with these folks:
Wide infrasternal angle = Sacral Nutation
And to make it easy fam, the reverse will be true for the narrows. A narrow infrasternal angle (<90 degrees), the anterior diaphragm is eccentric, and the posterior is concentric.
This visceral movement will result in a counternutated sacral position.
Narrow infrasternal angle = sacral counternutation
Given what we know about each sacral position, we can then relate how the contractile bias will be in each respective infrasternal angle (ISA) archetype:
Wide ISA = Sacral nutation = eccentric posterior pelvic floor + concentric anterior pelvic floor
Narrow ISA = Sacral counternutation = concentric posterior pelvic floor + eccentric anterior pelvic floor
Pelvic outlets and incontinence
Question: Can you please define what is anterior and posterior pelvic outlets and their role in incontinence and how should we approach them?
Answer: The outlet is the bottom ring of the pelvis. So if you drew a perimeter of the bottom of the pelvis, you’d get the outlet
Chop that perimeter in half (OUCH!), and you’d get the front part (anterior) and back part (posterior).
Fill ’em with muscle like we discussed in the last question, and you’d see what composes each. Anterior outlet houses anterior pelvic floor, and posterior outlet houses the posterior pelvic floor.
If there is a loss of dynamics in certain folks, that could be a contributing factor to incontinence. If I have reduced contractile options in the pelvic floor, sphincter control may not be as good as needed to keep ya stuff in.
Now it goes without saying, PLEASE GET CHECKED OUT if you have incontinence of any kind, as there can be some medical factors (e.g. cauda equina syndrome) that could cause this. But if you get checked out okay, then read on.
Theoretically, incontinence would happen when the downward pressure of the viscera would be so great that a release of the bowels or bladder would occur to help reduce the pressure. For me, this would start with coaching the stack, then ideally progressing through a full-depth squat, as this will allow one to pass through all ranges that the sacrum ought to be able to demonstrate.
Restoring pure nutation dynamics could also be useful aka getting your hinge on point.
Now all that side aside from improving these actions, it may be worthwhile working with a pelvic floor specialist, as sometimes internal work and cueing may be beneficial, and there may be local issues that need to be addressed. Clinically, I’ve found that if a client plateaus with a movement-based approach, then internal work seems to finish the job. Vice versa, if internal work isn’t cutting it, then maximizing breathing dynamics can be helpful. Ideally, you’d blend both disciplines.
Narrow infrasternal angle with pelvic floor dysfunction
Question: Hey Zac, do you have any tips on treating pelvic floor dysfunction? I’m a narrow infrasternal angle (ISA) with secondary compensations, doing the best I can to restore movement options. Anything more I can do to help this?
Answer: It’s hard to say without evaluating what the best bet would be, or what is meant by pelvic floor dysfunction. Of course, get checked out and consult with a pelvic floor specialist first to rule out any bad stuff.
But let’s say you’ve done that, things are gucci down there, but movement restrictions are the rate limiting step. Let’s also suppose this person is restricted EVERYWHERE.
Here is the process I would look into hitting up:
Step 1: Teach movement with less tension
The first key would be to get this person to move their body parts independently. When there is progressive compensation, there is a loss of relative motion between joints, so they essentially move more as one unit to complete an action. When you see a huge anterior pelvic tilt in a movement, that would be an example of this situation.
To begin teaching one to move their body independently, teaching the concept of moving with as little tension as possible is useful. The bigger muscle groups are less likely to contract like WHOA, “locking” everything in place.
These two foam roller rolling patterns are excellent starting points:
You can then progress to a full-body roll, but hella slow. The upper body roll is the pinnacle, fam beware:
Step 2: Work on the stack
Once you have some ability to create less tension when you move, it’s time to get your stack on track. For a narrow, I like teaching this in hooklying, as there is a bit more external rotation-bias, since that’s often limited in someone who is hella stiff everywhere. It’s also less end-range then say a Lewitt position.
Step 3: Progress the squat
Once you have the stack not whack, progressing someone down into a squat is going to be the show, as this movement will help clear up any posterior restrictions, which is common with this presentation.
The issue: someone who is limited everywhere can have a hard time getting the tuck in a bilateral stance.
The solution: offset your supreme clientele
The offset position induces just a lil’ bit of rotation in the mix, and having that small gradient can make the tuck WAY easier to achieve. This can be first achieved with a wall squat variation:
Then to get some depth, you can offset sink squat:
From here, you can take the training wheels off and add weight with a goblet squat:
I like to finish the last bit by using some weight to assist into the bottom, with an offset cheat clean:
Asymmetrical pelvic floor tightness
Question: How would you go about “fixing” a right posterior pelvic floor that is constantly tight in an asymmetric position?
Answer: If the right posterior pelvic floor is limited, there is often a loss of hip internal rotation on that side.
If internal rotation is gone, you…must…get…it.
I improve this motion in the following manner:
- Stack
- Drive adduction
- Progress the squat
- Turn left
Especially on the left turn, getting this turn in mid-depth ranges can help with increasing range of motion. An offset sink squat is a good choice:
Should I squeeze my pelvic floor when lifting heavy?
Question: Do you believe in contracting the pelvic floor for big lifts?
Answer: Not really, and the reason why is because, with high-performance activities, the internal cueing and cognitive load ought to be low. This could be counterproductive to maximizing output in this situation.
The best be? Get a full stack, inhale, and hold your breath (aka the valsalva maneuver).
Sum up
- A wide ISA has a concentric anterior pelvic floor (nutated sacrum), and a narrow ISA has a concentric posterior pelvic floor (counternutated sacrum)
- Incontinence (barring medical reasons) can be compounded with loss of pelvic floor dynamics. Working squatting and internal work can be useful for treatment
- Reduce tension, teach the stack, then progressing the squat can be a useful progression to maximizing movement options.
- If there is an asymmetrical position in the pelvis, you’ll want to drive pelvic rotation
- Pelvic floor contractions are not encouraged during high performance activities.