Category: All Things Rehab
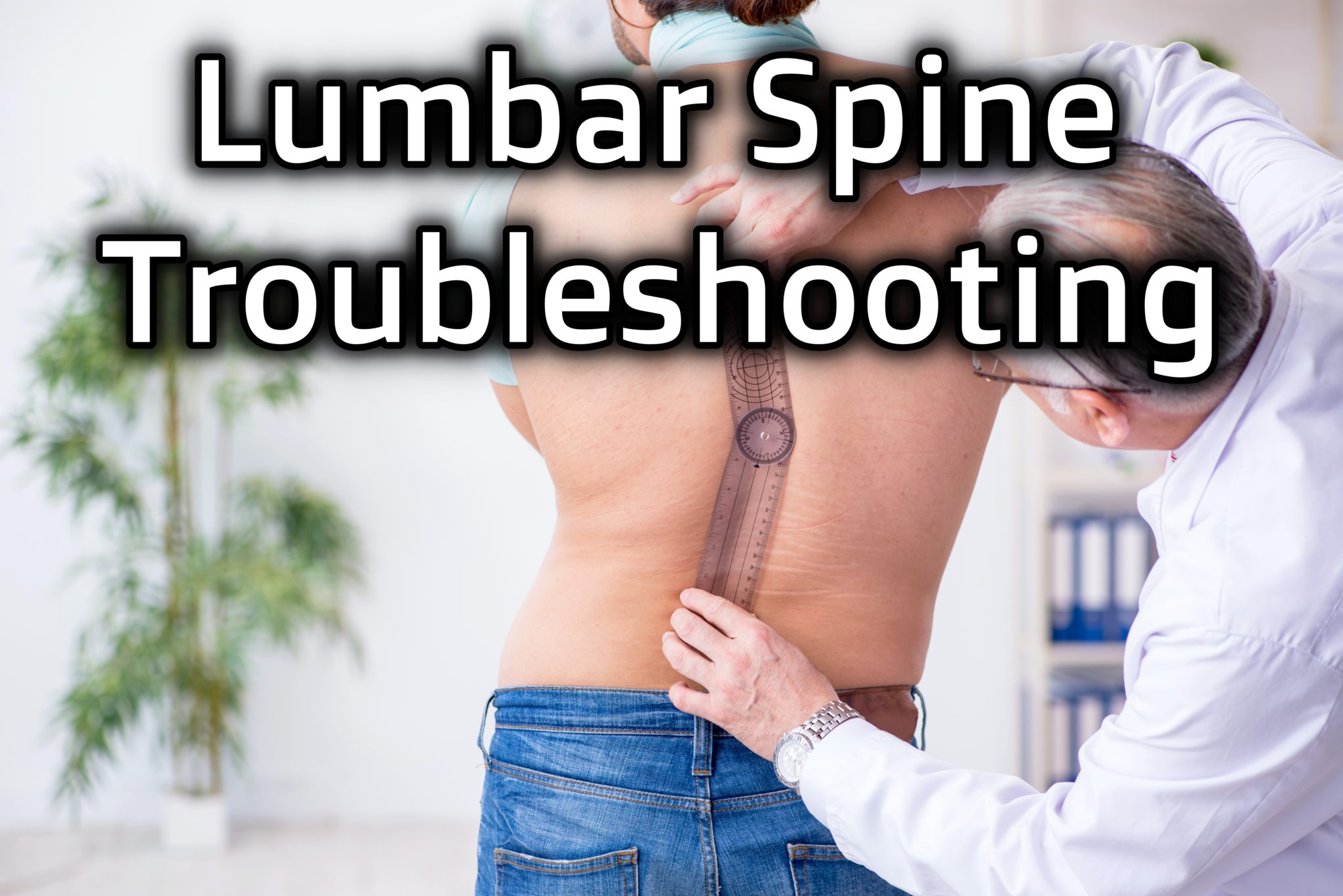
Lumbar Spine Troubleshooting
If you have someone who is flexion intolerant, has radicular symptoms, lateral shifts, and more, then you’ll want to check…

Hip Biomechanics in Movement
If you want clarification on how the hips work when you squat and shift, and navigate through common hip mobility…
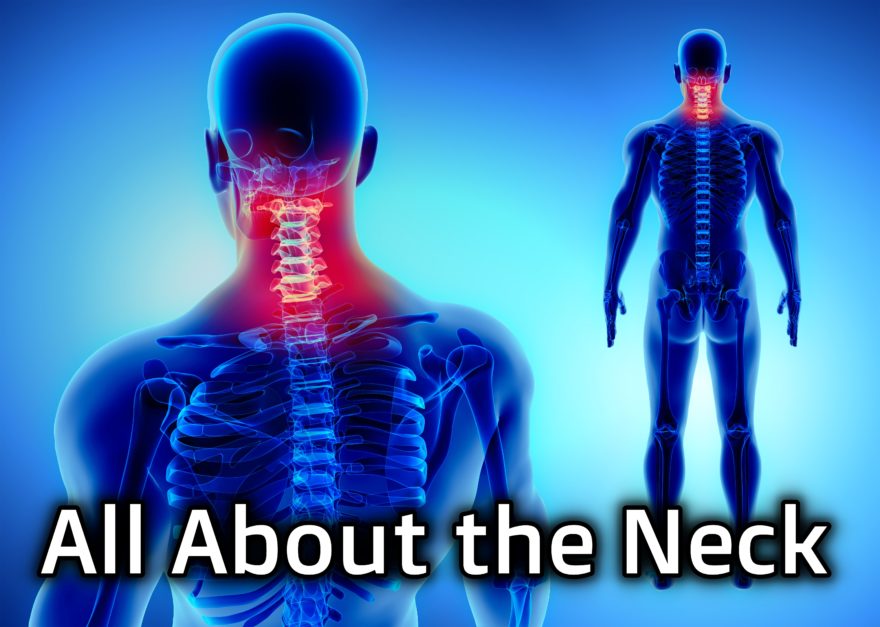
All About the Neck
A comprehensive look at cervical biomechanics and exercise The Wu-Tang clan once said “Protect Ya Neck,” but how in the…

Compensatory Movement Patterns
Know different postures you will see inside and out! It seems like there are a bazillion different types of postural…
How a Six Pack Affects Movement
A deep dive into abdominal wall compensations Movement Debrief Episode 120 is in the books. Below is a copy of…
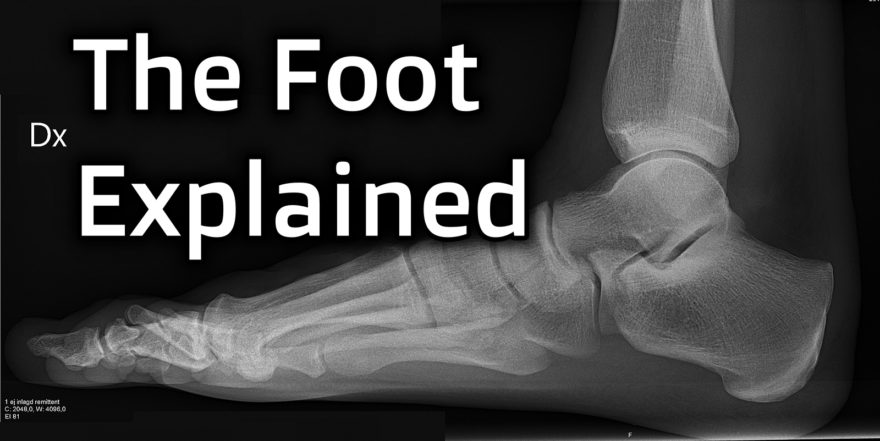
The Foot Explained
Biomechanics, compensation, and treatment of the foot Movement Debrief Episode 119 is in the books. Below is a copy of…

All About the Ribcage
Learn how reaching and improve upper body mobility Movement Debrief Episode 117 is in the books. Below is a copy…
Introduction to Orofacial Myofunctional Therapy Course Review
How improving tongue mobility can impact sleep and nasal breathing I hit a plateau. I was getting good results with…
Reaching: Theory and Practice
Learn how reaching and improve upper body mobility Movement Debrief Episode 116 is in the books. Below is a copy…
Hip Rotation Explained – Movement Debrief Episode 111
Movement Debrief Episode 111 is in the books. Below is a copy of the video for your viewing pleasure, and…

Is Spinal Flexion Bad? – Movement Debrief Episode 110
Movement Debrief Episode 110 is in the books. Below is a copy of the video for your viewing pleasure, and…

All About the Scapula – Movement Debrief Episode 109
Movement Debrief Episode 109 is in the books. Below is a copy of the video for your viewing pleasure, and…
The Unsexy Side of PT
Struggle with mouth breathing? Much of the stuff taught on my site focuses on maximizing your breathing skills from the…
Anterior Pelvic Orientation, Breathing During Squats and Deadlifts, and Handstands – Movement Debrief Episode 108
Movement Debrief Episode 108 is in the books. Below is a copy of the video for your viewing pleasure, and…
The Learning Process, The Axial Skeleton, and Squats – Rebel Performance Podcast
Are you struggling at structuring your learning? Or perhaps this whole inhalation and exhalation mechanics in regards to movement is…