
Table of Contents
If breathing exercises don’t change symptoms, what’s next?
Although exercises I teach do WONDERS for symptom relief, you don’t always get the incredible results that people show on social media.
Sometimes the results are mild.
Sometimes you even FAIL.
This case study I’m about to show you is an example of that.
Here, you’ll see that I get pretty solid changes on the table, but symptoms are minimally impacted.
What do you do then?
Watch the video and read the case report below to learn.
Case Overview
Chris is my social media czar and an awesome coach who both works with my personal clients and at our gym, Elevate.
A couple of weeks ago he was performing a front squat, had awkwardly caught the bar, and hurt below his left shoulder blade.
He’d feel better after a couple of days, would try to lift, pain would increase, and the cycle repeated.
When I saw him moving gingerly after Spikeball, I knew something was up.
His biggest aggravating factors were:
- Sleeping
- Any rotation or anti-rotation
- Worst in the morning
- Lifting
Things that made his pain better:
- End of day
- Lying on his back
I ended up taking a look at him and here were his objective tests:
Objective findings
Toe touch (%): 90
Squat (%): 76
LUMBAR
Rotation (L/R%): 10*/10*
Tenderness to palpation along the lateral ribcage and below the left scapula.
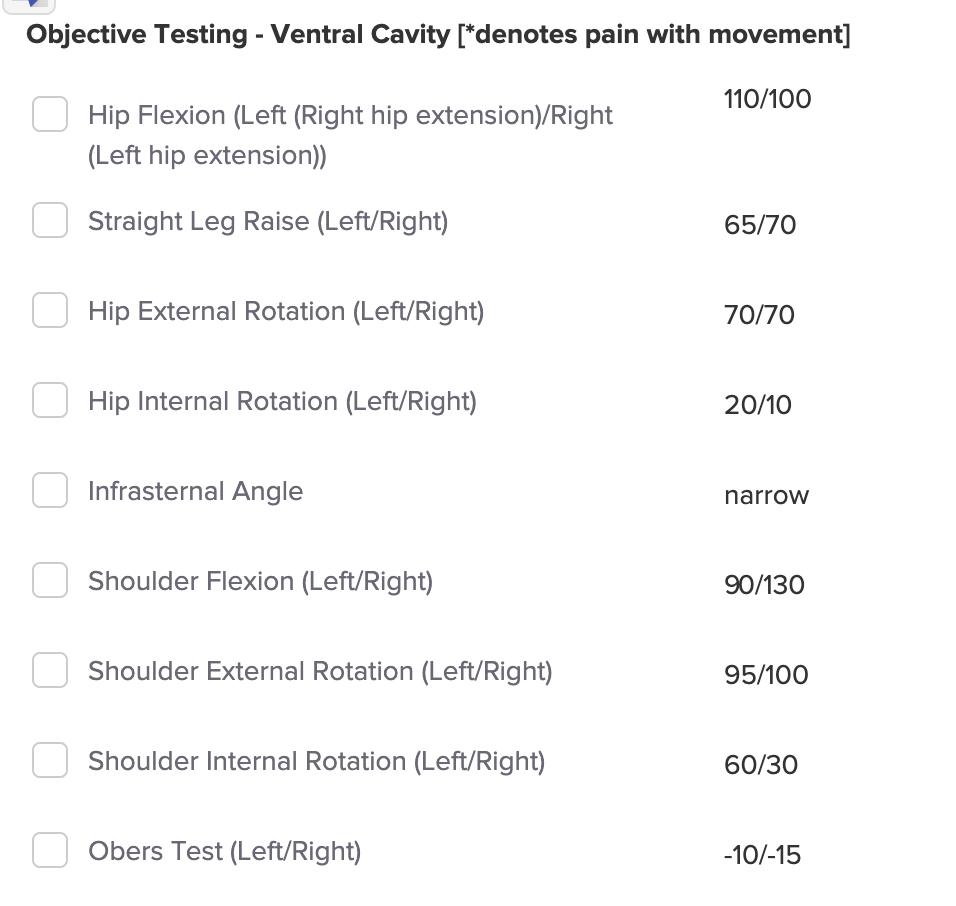
So Chris is a fairly classic narrow infrasternal angle presentation with the asymmetries indicating he is beginning a right turn.
What’s interesting is the discrepancy between his standing measures and table tests. The increased muscle activity needed to stand may contribute to the significant standing restrictions.
What does stand out to me measurement-wise is the significant left shoulder flexion loss. It could be that he has some increased muscle activity in the area in question that is “pushing” him to the right, hence the asymmetries. This will be an important test, especially considering symptom location.
The big concern here as well is that the pain is worse in the morning.
Usually, morning pain indicates an inflammatory process undergoing. Sleep “shuts off” inflammation. Upon awakening, those processes kick up into high gear.
Regardless, I decided to give it a go. The big keys we were going to focus on are:
- Stacking to make ISA dynamic
- Increasing internal rotation capabilities
- Driving left rotation
Here’s what I first went with.
Left offset walking wall squat (exercise 1)
I went with this move for the following reasons:
- Pushing hips backward will help Chris get some sacral nutation, which will help with internal rotation
- His chest facing downward will cause gravity to push air and abdominal contents more forward, increasing anterior expansion (needed for a narrow ISA)
- The offset on the left ought to improve leftward rotation, which hopefully will help with shoulder flexion
Results:
Here were the tests that changed after this exercise:
| Test | Left | Right |
| Standing Rotation | No change | No change |
| Hip Internal Rotation | 25º (+5º) | 20º (+10º) |
| Hip Flexion | 120º (+10º) | 120º (+20º) |
| Straight Leg Raise | 70º (+10º) | 65º (-5º) |
| Ober’s test | No change | -10º |
| Shoulder Internal Rotation | 80º (+20º) | 50º (+20º) |
| Shoulder Flexion | No change | No change |
Overall, some decent changes on the table.
We did get some overall improvements in internal rotation, but we aren’t as close as I would like. Because of that, we probably don’t have enough motion to push left rotation, which I hypothesize would be most helpful for symptom relief.
Unfortunately, his standing measures and shoulder flexion didn’t budge. I was also hesitant to give this move for home because it did aggravate his symptoms a bit.
Given these factors, I think continuing to emphasize the stack and increasing internal rotation is the way to go.
Frog breathing (exercise 2)
I went with this move for the following reasons:
- The wide arm/leg stance drives very small ranges of internal rotation (due to pressing into the ground) from an externally rotated position
- His chest facing downward will cause gravity to push air and abdominal contents more forward, increasing anterior expansion (needed for a narrow ISA)
- The prone position naturally increases lateral ribcage dimensions, helpful for stacking narrow ISAs.
Results:
Here were the tests that changed after this exercise (improvements are compared to results after the first exercise):
| Test | Left | Right |
| Standing Rotation | No change | No change |
| Hip Internal Rotation | 25º | 30º (+10º) |
| Hip Flexion | 120º | 120º |
| Straight Leg Raise | 70º | 65º |
| Ober’s test | No change | -10º |
| Shoulder Internal Rotation | 90º (+10º) | 50º |
| Shoulder Flexion | 120 (+30º) | 160 (+30º) |
Boom! We got some really nice changes regarding internal rotation. The change in right hip and left shoulder internal rotation, and left shoulder flexion indicated that we reduced some of the right turn bias that Chris has.
But sadly, standing measures continued to not change.
Here, I felt like we had enough internal rotation motion to drive left rotation.
Left sidelying same connect roll (exercise 3)
I went with this move for the following reasons:
- The block keeps the left arm and leg in a position where more left posterior expansion is biased, which is needed to drive left rotation
- Ground support will make it easier to attain this rotation
- Starting in sidelying reduces the amount of left rotational range that’s being expressed
Results:
Here were the tests that changed after this exercise (improvements are compared to results after the second exercise):
| Test | Left | Right |
| Standing Rotation | No change | No change |
| Hip Internal Rotation | 30º (+5º) | 30º |
| Hip Flexion | 120º | 120º |
| Straight Leg Raise | 70º | 65º |
| Ober’s test | No change | -10º |
| Shoulder Internal Rotation | 90º | 60º (+10º) |
| Shoulder Flexion | 120º | 160 |
Manual Therapy
I tried two techniques. The first was just a sidelying lateral ribcage expansion to see if I could help make the ISA more dynamic and just increase leftward space to drive more rotation. I then tried to replicate this in standing as well.
I also did a movement to recreate a hang to see if that could be another potential exercise.
Results:
After the ground-based manual, we got:
| Test | Left | Right |
| Standing Rotation | Mod improvement w/ less symptoms | Slight improvement w/ less symptoms |
| Hip Internal Rotation | 30º (+5º) | 30º |
| Hip Flexion | 120º | 120º |
| Straight Leg Raise | 70º | 65º |
| Shoulder Internal Rotation | 90º | 65º (+5º) |
| Shoulder Flexion | 155º (+35º) | 160 |
This was the first time the symptoms were less, with the biggest changes in standing rotation. Here we got a pretty significant improvement in symptoms and motion, though once my hands left, the motion didn’t stick.
I opted to have him tape in this position to see if that would alleviate symptoms in short term, and then I switched out the wall squat for a bar hang, which I thought better mimicked what I did manually.
Post-session debrief and recommendations
Although we got great changes on the table, none of these translated to meaningful changes to his standing measures, which were most painful.
The thing that led to the most symptom relief was manual therapy and assistance in standing, which is why I eventually recommended taping to see if that would help. But again, the changes were minor.
It is at this point that I felt it was wisest to address the elephant in the room: inflammation.
Because Chris really didn’t give himself adequate rest after the initial injury, my recommendations were to focus on giving himself a bit of time to let the inflammatory process run its course. Here were my recommendations:
- Do the moves
- Lay off lifting for one week. Move as much as you can comfortably
- Cardio would be okay
- Do anything that reduces inflammation
Chris followed these recommendations pretty well.
Chris’ outcome
A few days later, he worked with one of our massage therapists, Fern Garcia. Fern did various manual therapies and Chris had some significant symptom relief. Fern then recommended that Chris perform the moves I prescribed right after.
A few days after that, Chris was able to play spikeball pain-free. I encouraged him to ease back into lifting, emphasizing squats, and single-leg and single-arm exercises.
Sum up
As you can see, pain is complex, and improving available movement is only one part of the story. Here, we had to look at other factors that could be contributing to Chris’ problems.
To recap:
- Exhaust how much movement you can improve through exercise and manual therapy
- Provide palliative options to reduce symptoms short term
- If an inflammatory process is undergone, then provide recommendations to reduce inflammation
What cases have you struggled with? Comment below and let us know.