Tag: dentist
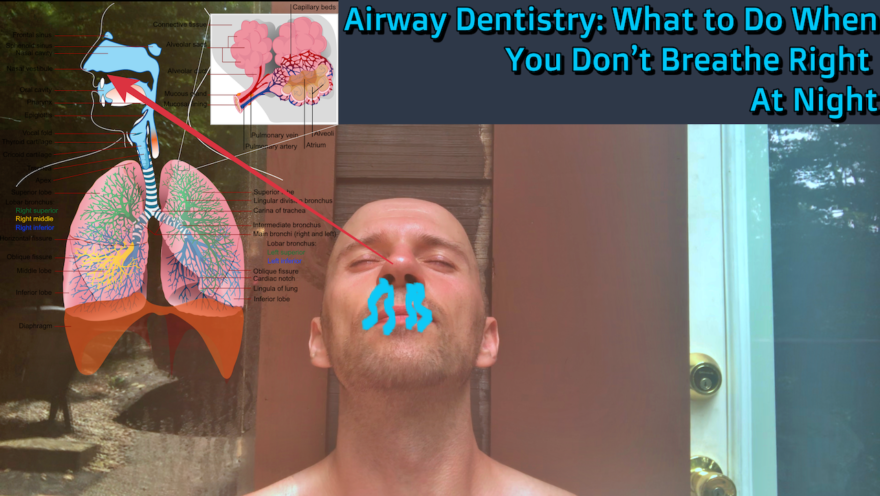
Airway Dentistry: What to Do When You Don’t Breathe Right At Night
If you are having trouble sleeping, snore at night, or mouth breathe like none other, you definitely have to listen…
Geriatrics, Pain with Breathing, and Dentists – Movement Debrief Episode 99
Movement Debrief Episode 99 is in the books. Below is a copy of the video for your viewing pleasure, and…
July 2018 Links and Review
Every week, my newsletter subscribers get links to some of the goodies that I’ve come across on the internets. Here…
Acute Pain, Dead Hangs, and Occlusion – Movement Debrief Episode 40
Movement Debrief Episode 40 is in the books. Below is a copy of the video for your viewing pleasure, and…
Course Notes: PRI Cervical Revolution
Where are all the People? I recently made the trek to Vermont for the first rendition of PRI’s Cervical Revolution…
Course Notes: The Last Craniocervical Mandibular Restoration Evahhhhh
You’d Think I’d Learn it the First Time Around You’d think, but CCM is one of the hardest PRI courses…
A Fly on the Wall of the Hruska Clinic
The Saga Continues This post is way overdue, but a lot has been going on in life. I have just…
Treatment at the Hruska Clinic: PRI Dentistry and Vision
For part 1, click here For part 3, click here Jaws will Drop I’m in the dentist chair, The room…
Treatment at the Hruska Clinic – Initial Evaluation
For part 2, click here. For part 3, click here. “Do you produce enough saliva?” That was the first interview…